Download
1 / 26
260 likes | 410 Views
Ventilator Strategies in Donor Management Live Webinar. Moderator: Nancy Knudsen, MD Summit Co-Chair, Professor of Anesthesiology, Assistant Professor of Surgery, Co-Medical Director Surgical Intensive Care Unit (SICU), Duke Medical Center, NC.

E N D
Ventilator Strategies in Donor Management Live Webinar Moderator: Nancy Knudsen, MD Summit Co-Chair, Professor of Anesthesiology, Assistant Professor of Surgery, Co-Medical Director Surgical Intensive Care Unit (SICU), Duke Medical Center, NC
From futility to fruition: What can I do in the ICU to maximize donor lung potential? Lydia Lam, MD Surgical Critical Care, Univ of Southern California Dan Lebovitz, MD Pediatric Critical Care, Akron Children’s Hospital Medical Director LifeBanc
Why are we concentrating on lungs? • Increasing number of ptsneeding lung transplant • Static number of lung donors • Shortage of good quality lung donors • Utilization rates of donor lung ~15% Strategies for safe donor expansion: donor management, donations after cardiac death, ex-vivo lung perfusion. Cypel, M.CurrOpin Organ Transplant 2013, 18:513-517
Waiting as of 9/24/2013 4:48pm EST1630 pts for lungs, 48 pts for heart/lung
Quick Review Lung transplantation is often the only treatment for end stage lung disease Limited availability of lungs for transplantation leads to deaths on the waiting list ~ 8000 deceased donors annually in US only ~20% of these are lung donors Donor lungs are declined for numerous reasons most importantly PaO2 /FiO2 ratio < 300 Volume cycled/ controlled modes of ventilation with TV ~10 ml/kg, 100% FiO2, PEEP 5
Patient Arrival to ER • HPI: 22yoM s/p GSW to head. Pt. was found down at home w/GSW to head w/exposed brain matter. No other wounds found at site. Another female victim was also found dead at the scene. • A-abnormal, not protecting • B-abnormal, BVM, RR12 O2Sat 99%. • C-abnormal, HR 90, BP 81/29, Temp UTO • D-GCS 4, E1, V1, M2. Pupils fixed and dilated. Posturing decerebrate. Gag present initially. Sensory UTA.
Copious, pulsatile bleeding from GSW • What do you do?
Patient Course in ICU • Admitted at 8:30am • 11am • Despite resuscitative fluids and transfusions, rapidly declined • FFP 8 u and 3 PRBC via rapid transfuser • Pressors: DA20, epi 20, T4 10, VP 0.04 • Hypotensive to 50/20 with transient improvement after epi amp given • 100% FiO2 with ABG 7.25, pCO2 75, pO2 28
Consult OPO • Coded several times • OPO coordinator present and “signed off” at this time due to patient “coding” • What do you do?
Catastrophic Brain Injured Does NOT Improve Improve Donor Not a Donor
Respiratory Effects Primary pulmonary disease Trauma Aspiration Pneumonia Neurogenic pulmonary edema Cardiogenic pulmonary edema Ventilator-associated barotrauma
Multi Trauma • Hemorrhage • Hemorrhage • Hemorrhage • Hemorrhage • Resuscitation…..
Multi Trauma • Aspiration • Pneumonitis • Lung contusions • Displaced rib fractures • Pulmonary edema
Complications of brain death Salim A, et al. Am Surgeon, 2006
Role of Brain Death in Donor Lung Injury Neurogenic Pulmonary Edema “Blast Injury Theory”→ Hemodynamic mechanism Sympathetic surge Transient massive ↑ hydrostatic pressure with structural damage to capillary endothelium Sympathetic alteration of capillary permeability Alvonitis Transplantation 2003
Lungs • ~15% brain dead patients with retrieval • Lower CVP • Steroids have shown to improve function
Early Donor Management Increases the Retrieval Rate of Lungs for Transplantation • Randomized controlled trial • Conclusions • Early active management of lung donors increases yield • Steroid administration reduces lung water accumulation Venkateswaran RV, et al. Ann ThoracSurg 2008
Catastrophic Brain Injured Does NOT Improve Improve Donor Not a Donor
Vent Management Donor or Not • Treat cofounding variables • Ventilator bundle • ARDSnet • Minimize barotrauma • Improve oxygenation • Hypervigilance • Especially important in DCD patient as OPO has no role
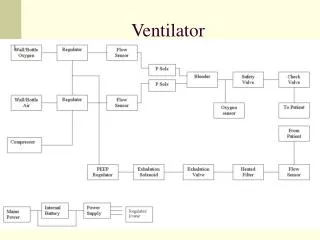
Airway Pressure Release VentilationAPRV • Pressure control mode • High constant positive airway pressure • Intermittent releases • Spontaneous breathing • Paralysis not required
APRV Inspiration Expiration Frawley PM, Habashi NM. AACN Clin Issues 2001