Download
1 / 13
140 likes | 413 Views
Why study statins?. #1 & #2 selling drugs in the world are statins – these two drugs account for 5% of the entire United States spending on drugs ($11.2 billion dollars), since Heart disease is the #1 killer in industrialized countries The poor prognosis of homozygous FH patients.

E N D
Why study statins? • #1 & #2 selling drugs in the world are statins – these two drugs account for 5% of the entire United States spending on drugs ($11.2 billion dollars), since • Heart disease is the #1 killer in industrialized countries • The poor prognosis of homozygous FH patients
Why study statins? • Interesting clinical trial (hi)story – some highlights • 100 years ago Virchow discovers “atheroma” • 1985: NIH initiates public health initiative to educate patients and doctors about dangers of hypercholesterolemia • First statins caused cataracts and did not reduce plasma cholesterol in rats – why? • Crazy synthesis of mevinolin, which works for heterozygous FH • Mevinolin is twice withdrawn from clinical studies Mevinolin - further proof fermentation is a good thing
Why study statins? • Classic example of a simple biochemical intervention that turned out to be much more complicated than anyone thought…. • Hence, the papers
Goal of the study How is lovastatin causing a decrease in plasma LDL concentration?
Their approach - eliminate a possible mechanism for lovastatin • Two possible mechanisms of action: • ↓LDL by ↓formation of apo-B • ↑uptake of VLDL remnants due to ↑LDLR, so fewer VLDL remnants to be converted to LDL No receptors means no VLDL or LDL clearance by liver – if cholesterol is lowered, lovastatin is decreasing production of lipoproteins
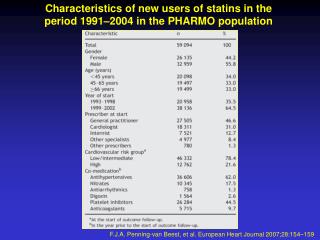
The patients • Requirements: 1) severe hypercholesterolemia 2) extremely low LDL-R activity in skin fibroblasts 3) evidence of heterozygous FH in both parents * Normal cholesterol levels are <200mg/dL; studies show levels of 240 mg/dL put you at 2x risk for coronary events Study protocol: 4 wks of control, 6 wks of lovastatin treatment under controlled conditions
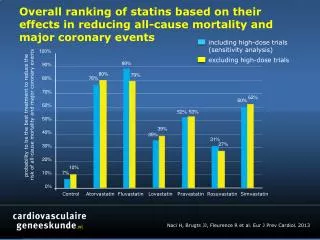
Conclusions • ↓LDL must be due to LDL-R activity • ↑LDL in homozygous FH probably due to lack of uptake of VLDL by liver; transfer to LDL by lipoprotein lipase, NOT to ↑ apo-B synthesis in liver • A very significant decrease in plasma [VLDL] – why?
Two theories, neither satisfactory • Theory 1: partial inhibition of cholesterol synthesis means less VLDL • Problem: rate of formation of LDL was not reduced; this is not the mechanism of action of lovastatin • Theory 2: Small residue of LDL-R activity removes remnants, but not LDL • Problem: they’ve established these patients have essential NO receptor activity and their experiment is based on a lack of receptor activity
Who approved this IRB? Is this the best way to answer their question?
Points to consider • Isn’t an animal receptor KO model essentially the same as the human homozygous FH model? Has this experiment already been done? • Is it appropriate to use human subjects to confirm a drug does NOT work? • What if you take them off their current treatment for months? • What if you feed them a diet that further complicates their illness? • What if they are six-year-old children? • What if previous studies seem to indicate that the drug will not work? • What if you will be using radioactive iodine isotopes? (invasiveness of study) • How would you pitch this study to a family? (i.e., this probably won’t work, but what’s important is why?) • Is obtaining consent from a 6-yr-old feasible? • Does the prognosis of the patients make a difference?