Download
1 / 33
350 likes | 642 Views
COMMON VIRAL INFECTIONS. Dr.H.N.Sarker MBBS. FCPS.MACP(USA) Assistant professor Medicine. Topics. Introduction Clinical syndromes caused by viruses SYSTEMIC VIRAL INFECTIONS. Introduction.

E N D
COMMON VIRAL INFECTIONS Dr.H.N.Sarker MBBS. FCPS.MACP(USA) Assistant professor Medicine
Topics • Introduction • Clinical syndromes caused by viruses • SYSTEMIC VIRAL INFECTIONS
Introduction • Viruses are simple infectious agents consisting of a portion of genetic material, RNA or DNA, enclosed in a protein coat. • They are essentially intracellular and cannot exist in a free-living state, needing to infect host cells to survive.
Clinical syndromes caused by viruses • Classification/viruses involved Clinical syndromes • DNA VIRUSES(PHAPH) • Poxviruses(Variola) Smallpox • Herpes viruses • Herpes simplex types 1 and 2 Acute/recurrent vesicular rash(Herpes labialis) • Varicella zoster Chickenpox/shingles
Clinical syndromes caused by viruses • Cytomegalovirus Acute/recurrent hepatorenal infection • Epstein-Barr virus Infectious mononucleosis Burkitt'slymphoma Nasopharyngeal carcinom
Clinical syndromes caused by viruses • Human erythrovirus 19 Erythema infectiosum • Adenoviruses Upper respiratory tract infection/pharyngitis Acute diarrhoea
Papovaviruses • Human papillomavirus Common wart • Polyoma (human BK and JC) Progressive multifocal leucoencephalopathy Hepadnavirus Hepatitis B
Clinical syndromes caused by viruses • RNA VIRUSES(MRTCRP) • Myxovirus- OrthomyxovirusesInfluenzaA,B ParamyxovirusesMeasles Mumps Respiratory syncytial virus
Clinical syndromes caused by viruses • RetrovirusesHIV-1 and 2HIV infection syndrome/AIDS • TogavirusesRubella German measles Dengue fever
Clinical syndromes caused by viruses Calicivirus Hepatitis-E Rhabdoviruses Rabies Picornaviruses Poliovirus polio Coxsackie viruses pericarditis
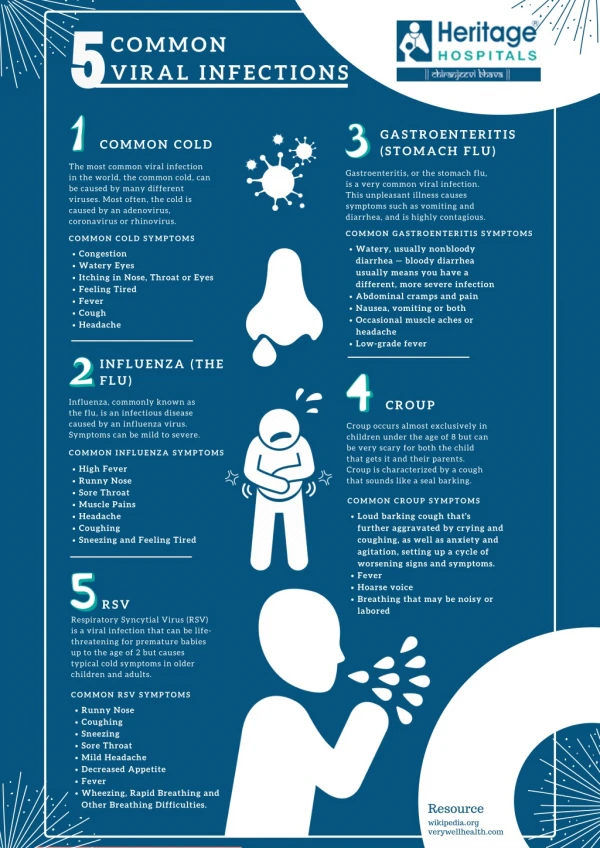
SYSTEMIC VIRAL INFECTIONS • INFLUENZA • INFECTIOUS MONONUCLEOSIS (IM) • ACQUIRED CYTOMEGALOVIRUS INFECTION • DENGUE • YELLOW FEVER
INFLUENZA • A specific acute illness caused by a group of myxoviruses • Aetiology: Influenza A and B virus
INFLUENZA • Clinical feature: Sudden onset of pyrexia Generalized ache and pains , headache. Anorexia , nausea and vomiting
INFLUENZA Harsh nonproductive cough Acute symptoms subside within 3-5 days but may be followed by post influenza asthenia which may persist for several weeks.
INFLUENZA • Complication: Most patients donot develop complication. Trachitis, bronchitis, bronchiolitis , Bronchopneumonia Secondary bacterial invasion by Streptococcus pneumoniae, H. influenzae, Staph. aureus.
INFLUENZA • Complication: Rare Toxic cardiomyopathy may cause sudden death Encephalitis Demyelinating encephalopathy Peripheral neuropathy
INFLUENZA • Management: Bed rest till fever subsides Parectamol .5-1 gm(1-2 tab) 4-6 hrly Pholcodine 5-10 mg 6-8 hrly Antibiotic if secondary bacterial infection.
INFECTIOUS MONONUCLEOSIS (IM) • INFECTIOUS MONONUCLEOSIS (IM) is caused by the Epstein-Barr virus (EBV), a gamma herpes virus.
Virology and epidemiology • Epstein-Barr virus (EBV) is a B lymphotropic human herpes virus which is worldwide in distribution. • Primary infection with EBV which occurs during childhood is usually subclinical. • Between 25-70 % of adolescents are usually subclinical.
Virology and epidemiology • Between 25-70 % of adolescents and adults who undergo a primary EBV infection develop the clinical syndrome of infectious mononucleosis. • Saliva is the main means of spread, either by droplet infection or environmental contamination in childhood, or by kissing among adolescents and adults.
Clinical features • Infectious mononucleosis is defined by the clinical triad of fever, lymphadenopathy, and pharyngitis • combined with the transient appearance of heterophil antibodies and an atypical lymphocytosis.
Clinical features • Other features- splenomegaly, palatal petechiae, periorbital oedema, clinical or biochemical evidence of hepatitis, and a non-specific rash.
Diagnosis • Diagnosed by the clinical triad of fever, lymphadenopathy, and pharyngitis in typical age group(10-30 yrs). • combined with an atypical lymphocytosis.(20% or more of peripheral lymphocytes must have an atypical morphology). and
Diagnosis • the transient appearance of heterophil antibodies by 1.the classical Paul-Bunnell titration Or 2. a more convenient slide test such as the 'Monospot'.
Diagnosis • Specific EBV serology (immunofluorescence) can be used to confirm the diagnosis if necessary. • antiviral capsid (VCA) antibodies in the IgM class • antibodies to EBV early antigen (EA) • absent antibodies to EBV nuclear antigen (anti-EBNA).
COMPLICATIONS • Common • Severe pharyngeal oedema • Antibiotic-induced rash • Chronic fatigue syndrome (10%)
COMPLICATIONS Uncommon Neurological Cranial nerve palsies Polyneuritis Transverse myelitis Meningoencephalitis Haematological Haemolytic anaemia Thrombocytopenia
COMPLICATIONS • Renal Glomerulonephritis Interstitial nephritis • Cardiac Myocarditis Pericarditis • Pulmonary Interstitial pneumonitis
COMPLICATIONS • Rare Ruptured spleen Respiratory obstruction Arthritis Agranulocytosis Agammaglobulinaemia
Management • Treatment is largely symptomatic: aspirin gargles to relieve a sore throat. If a throat culture yields a β-haemolytic streptococcus, a course of erythromycin should be prescribed.
Management Amoxicillin and similar semi-synthetic penicillins should be avoided because they commonly induce a maculo-papular rash in patients with IM.
Management • When pharyngeal oedema is severe a short course of corticosteroids, e.g. prednisolone 30 mg daily for 5 days, may help to relieve the swelling.