Download

1 / 43
530 likes | 844 Views
Future Directions in Transcatheter Aortic Valve Replacement (TAVR) Therapies. Sandeep Nathan, MD, MSc , FACC, FSCAI Assistant Professor of Medicine Director, Interventional Cardiology Fellowship Program Director, Interventional Cardiology Research & Education

E N D
Future Directions in Transcatheter Aortic Valve Replacement (TAVR) Therapies Sandeep Nathan, MD, MSc, FACC, FSCAI Assistant Professor of Medicine Director, Interventional Cardiology Fellowship Program Director, Interventional Cardiology Research & Education University of Chicago Medical Center Chicago, IL
Disclosures • Consulting / Honoraria Sanofi Aventis • Merck, Inc. • Medtronic, Inc. • Advisory panel Daiichi Sankyo • Ortho McNeil • Grant support Accumetrics, Inc • Equity None * Investigational (non-FDA approved) technologies will be discussed during this presentation.
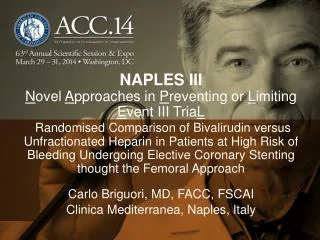
TAVI – PARTNER B Symptomatic Severe Aortic Stenosis ASSESSMENT: High-Risk AVR Candidate 3,105 Total Patients Screened Total = 1,057 patients High-Risk Inoperable n = 358 n = 699 2 Parallel Trials: Individually Powered ASSESSMENT: Transfemoral Access ASSESSMENT: Transfemoral Access High-Risk TA High-Risk TF 1:1 Randomization 1:1 Randomization 1:1 Randomization TF TAVR AVR TA TAVR AVR TF TAVR n = 179 Standard Therapy n = 179 VS VS VS Primary Endpoint: All-Cause Mortality Over Length of Trial (Superiority) Primary Endpoint: All-Cause Mortality (1 yr)(Non-inferiority)
ASSESSMENT: Transfemoral Access Yes No 1:1 Randomization Not In Study N = 179 N = 179 TF TAVR Standard Therapy VS Primary Endpoint: All-Cause Mortality Over Length of Trial (Superiority) Co-Primary Endpoint: Composite of All-Cause Mortalityand Repeat Hospitalization (Superiority) TAVI – PARTNER A Symptomatic Severe Aortic Stenosis ASSESSMENT: High-Risk AVR Candidate 3,105 Total Patients Screened Total = 1,057 patients High-Risk Inoperable N = 358 N = 699 2 Parallel Trials: Individually Powered ASSESSMENT: Transfemoral Access Yes No Transapical (TA) Transfemoral (TF) 1:1 Randomization 1:1 Randomization N = 244 N = 248 N = 104 N = 103 TF TAVR AVR TA TAVR AVR VS VS Primary Endpoint: All-Cause Mortality at 1 yr(Non-inferiority)
QOL assessment via KCCQ Kansas City Cardiomyopathy Questionnaire • Clinically Important Change • Small = 5 points • Moderate = 10 points • Large = 20 points Am Heart J. 2005;150:707-15.
QOL assessment via KCCQ Cohort A – Transfemoral subgroup
QOL assessment via KCCQ Cohort A – Transapical subgroup
So what’s on the wish list? Reimbursement policy for TAVR
TAVR wish list DATA 1. Long-term mortality data 2. Implication of stroke risk 3. Long-term performance data in Cohort A patients 4. Additional cost-effectiveness analyses 5. Implication of post-TAVR AI DEVICE 1. Lower profile devices 2. Repositionable devices 3. Retrievable devices 4. Paravalvular leak 5. Delivery system options 6. Eliminate need for pacing 7. Embolic protection 8. Deflectable delivery systems
TAVR: Present & future Edwards Sapien XT (2nd generation) 18/19 Fr with NovoFlex delivery system Medtronic Engager TA valve (Ventor Embracer) St. Jude Medical Portico valve Edwards Sapien THV (1st generation) 22/24 Fr with RetroFlex 3 delivery system Boston Scientific Lotus self-exp valve (Sadra Lotus) JenaValve Medtronic CoreValve
SapienTMvalve refinements * Investigational devices * Long-term clinical impact of Edwards tissue treatment has not been evaluated
SapienTMvalve refinements The blue flex catheter of both the NovaFlex and NovaFlex+ delivery systems is designed to stabilize the balloon shaft during valve deployment. The 360º Flex Tip design of the NovaFlex+ system provides tighter balloon shaft support for accurate deployment of the Edwards SAPIEN XT transcatheter heart valve and provides for easier valve alignment. The NovaFlex+ balloon tip has been shortened by 3mm to minimize the amount of material in the left ventricle.
Medtronic CoreValveTM • 18 Fr delivery system • Transfemoral or subclavian delivery • Repositionable, self-expanding system • Perhaps greater need for pacing afterwards
CoreValveTM– design modifications Anti-mineralization treatment Recapture & repositioning CE Mark for subclavian delivery Decreasing size
Medtronic Engager TM technology Design goals of Engager TM transapical TAVI platform* 1. Decrease risk of paravalvular leaks 2. Minimize coronary obstruction 3. Different anchoring than radial force alone 4. Allow anatomical positioning 5. Ability to reposition device * Previously known as Ventor Embracer TM
Medtronic Engager TM technology Delivery system Gen 3.0
Medtronic Engager TM technology Steps of deployment
Medtronic Engager TM FIM data * European (CE mark) pivotal clinical trial currently underway EHJ. In press
Sadra Lotus TM valve system Sadra LotusTM valve components and function
St. Jude Medical Portico TM valve FIM human implant: June 7, 2011
St. Jude Medical Portico TM valve * Long-term clinical impact of St. Jude anticalcification treatment has not been evaluated
St. Jude Medical Portico TM valve • Flexible, trackabletransfemoral delivery system • Sheathlesstransapical delivery system
St. Jude Medical Portico TM valve Timeline for investigative program and potential approval
JenaValveTMtransapical valve CE-Marked Transapical Valve System www.jenavalve.de
JenaValveTMtransapical valve www.jenavalve.de
JenaValveTMtransapical valve Clinical data (CE Mark Trial) www.jenavalve.de
JenaValveTMtransapical valve www.jenavalve.de
TAVR “roadmap” document Journal of the American College of Cardiology (2012), doi: 10.1016/j.jacc.2012.01.001.
CMS coverage of TAVR • Per CMS draft memo regarding national coverage determination (NCD), TAVR will be covered only for the treatment of severe symptomatic aortic-valve stenosis and the following five conditions must be met: • The procedure is performed for an approved indication with a valve and implantation system that has received FDA approval for this indication. • Two cardiac surgeons have evaluated the patient's suitability for open valve-replacement surgery. • The procedure is performed in a facility that meets certain requirements with regard to surgical and interventional cardiology expertise. In addition, institutions with prior TAVR experience must participate in ongoing trials or postapproval studies, and all centers performing TAVR must commit to the "heart-team" concept and enroll in a prospective national TAVR study. • TAVR must be carried out by sufficiently qualified and experienced physicians. • The treating team must participate in a national registry that enrolls TAVR patients and tracks the following outcomes: major stroke; all-cause mortality; minor stroke/transient ischemic attack; major vascular events; and acute renal injury. www.theheart.org. Accessed February 3, 2012
What can we expect for TAVR in the US? • Lower profile devices • Repositionable / retrievable devices • Enhanced & deflectable delivery system / release mechanism options • Embolic protection • Deflectable delivery systems • Learning curve • CMS / FDA oversight and guidelines • Mandatory reporting of data and performance metrics



![T. Lau, MD, FRCPC [psych], MSc., Assistant Professor, Faculty of Medicine, UNIVERSITY OF OTTAWA](https://cdn1.slideserve.com/3370549/slide1-dt.jpg)