Download
1 / 1
10 likes | 188 Views
Nitric Oxide And Soluble Lectin -like Oxidized LDL Receptor - 1 (sLOX-1) As Markers Of Neurovascular Oxidative Stress In Acute Stroke. Srikwan K., Muengtaweepongsa S.,MD, Suwanprasert K.,Ph.D. Faculty of Medicine, Thammasat University, Pathumthani, Thailand 12120.

E N D
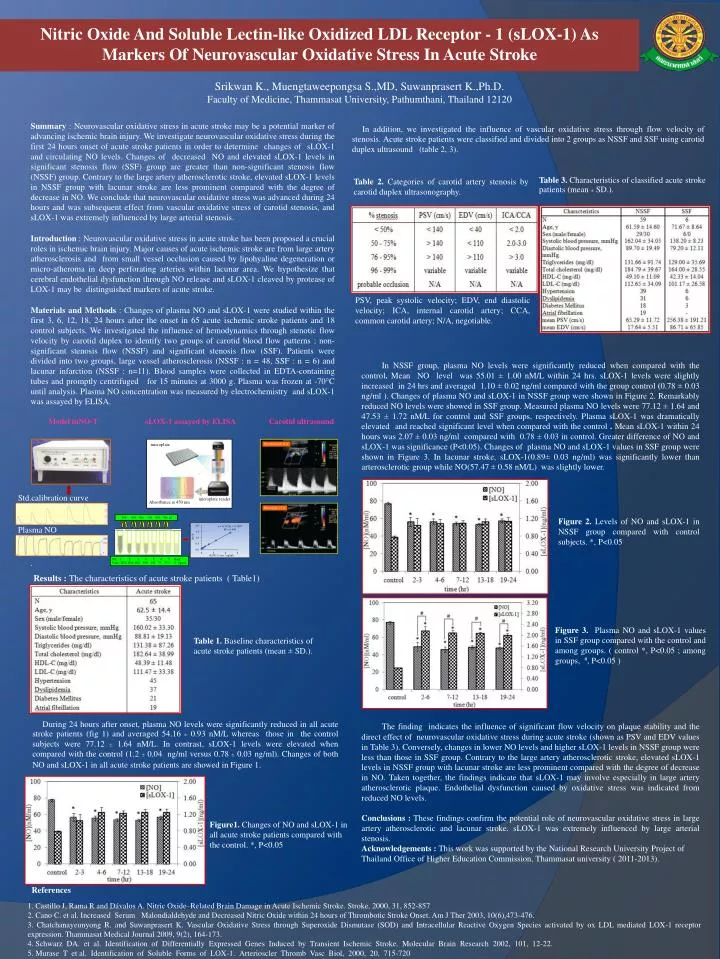
Nitric Oxide And Soluble Lectin-like Oxidized LDL Receptor - 1 (sLOX-1) As Markers Of Neurovascular Oxidative Stress In Acute Stroke Srikwan K., Muengtaweepongsa S.,MD, Suwanprasert K.,Ph.D. Faculty of Medicine, Thammasat University, Pathumthani, Thailand 12120 Summary : Neurovascular oxidative stress in acute stroke may be a potential marker of advancing ischemic brain injury. We investigate neurovascular oxidative stress during the first 24 hours onset of acute stroke patients in order to determine changes of sLOX-1 and circulating NO levels. Changes of decreased NO and elevated sLOX-1 levels in significant stenosis flow (SSF) group are greater than non-significant stenosis flow (NSSF) group. Contrary to the large artery atherosclerotic stroke, elevated sLOX-1 levels in NSSF group with lacunar stroke are less prominent compared with the degree of decrease in NO. We conclude that neurovascular oxidative stress was advanced during 24 hours and was subsequent effect from vascular oxidative stress of carotid stenosis, and sLOX-1 was extremely influenced by large arterial stenosis. Introduction : Neurovascular oxidative stress in acute stroke has been proposed a crucial roles in ischemic brain injury. Major causes of acute ischemic stroke are from large artery atherosclerosis and from small vessel occlusion caused by lipohyaline degeneration or micro-atheroma in deep perforating arteries within lacunar area. We hypothesize that cerebral endothelial dysfunction through NO release and sLOX-1 cleaved by protease of LOX-1 may be distinguished markers of acute stroke. Materials and Methods : Changes of plasma NO and sLOX-1 were studied within the first 3, 6, 12, 18, 24 hours after the onset in 65 acute ischemic stroke patients and 18 control subjects. We investigated the influence of hemodynamics through stenotic flow velocity by carotid duplex to identify two groups of carotid blood flow patterns ; non-significant stenosis flow (NSSF) and significant stenosis flow (SSF). Patients were divided into two groups, large vessel atherosclerosis (NSSF : n = 48, SSF : n = 6) and lacunar infarction (NSSF : n=11). Blood samples were collected in EDTA-containing tubes and promptly centrifuged for 15 minutes at 3000 g. Plasma was frozen at -70°C until analysis. Plasma NO concentration was measured by electrochemistry and sLOX-1 was assayed by ELISA. Model inNO-T sLOX-1 assayed by ELISA Carotid ultrasound . In addition, we investigated the influence of vascular oxidative stress through flow velocity of stenosis. Acute stroke patients were classified and divided into 2 groups as NSSF and SSF using carotid duplex ultrasound (table 2, 3). Table 3. Characteristics of classified acute stroke patients (mean ± SD.). Table 2. Categories of carotid artery stenosis by carotid duplex ultrasonography. PSV, peak systolic velocity; EDV, end diastolic velocity; ICA, internal carotid artery; CCA, common carotid artery; N/A, negotiable. In NSSF group, plasma NO levels were significantly reduced when compared with the control. Mean NO level was 55.01 ± 1.00 nM/L within 24 hrs. sLOX-1 levels were slightly increased in 24 hrs and averaged 1.10 ± 0.02 ng/ml compared with the group control (0.78 ± 0.03 ng/ml ). Changes of plasma NO and sLOX-1 in NSSF group were shown in Figure 2. Remarkably reduced NO levels were showed in SSF group. Measured plasma NO levels were 77.12 ± 1.64 and 47.53 ± 1.72 nM/L for control and SSF groups, respectively. Plasma sLOX-1 was dramatically elevated and reached significant level when compared with the control . Mean sLOX-1 within 24 hours was 2.07 ± 0.03 ng/ml compared with 0.78 ± 0.03 in control. Greater difference of NO and sLOX-1 was significance (P<0.05). Changes of plasma NO and sLOX-1 values in SSF group were shown in Figure 3. In lacunar stroke, sLOX-1(0.89± 0.03 ng/ml) was significantly lower than arterosclerotic group while NO(57.47 ± 0.58 nM/L) was slightly lower. The finding indicates the influence of significant flow velocity on plaque stability and the direct effect of neurovascular oxidative stress during acute stroke (shown as PSV and EDV values in Table 3). Conversely, changes in lower NO levels and higher sLOX-1 levels in NSSF group were less than those in SSFgroup. Contrary to the large artery atherosclerotic stroke, elevated sLOX-1 levels in NSSF group with lacunar stroke are less prominent compared with the degree of decrease in NO. Taken together, the findings indicate that sLOX-1 may involve especially in large artery atherosclerotic plaque. Endothelial dysfunction caused by oxidative stress was indicated from reduced NO levels. Conclusions : These findings confirm the potential role of neurovascular oxidative stress in large artery atherosclerotic and lacunar stroke. sLOX-1 was extremely influenced by large arterial stenosis. Acknowledgements : This work was supported by the National Research University Project of Thailand Office of Higher Education Commission, Thammasat university ( 2011-2013). microplate Proximal right ICA Std.calibration curve microplate reader Absorbance at 450 nm Distal right CCA 300 300 300 300 300 300 μl Figure 2. Levels of NO and sLOX-1 in NSSF group compared with control subjects. *, P<0.05 Plasma NO Std. 1 2 3 4 5 6 7 blank Conc. 2400 1200 600 300 150 75 37.5 0 pg/ml Results : The characteristics of acute stroke patients ( Table1) Figure 3. Plasma NO and sLOX-1 values in SSF group compared with the control and among groups. ( control *, P<0.05 ; among groups, #, P<0.05 ) Table 1. Baseline characteristics of acute stroke patients (mean ± SD.). During 24 hours after onset, plasma NO levels were significantly reduced in all acute stroke patients (fig 1) and averaged 54.16 ± 0.93 nM/L whereas those in the control subjects were 77.12 ± 1.64 nM/L. In contrast, sLOX-1 levels were elevated when compared with the control (1.2 ± 0.04 ng/ml versus 0.78 ± 0.03 ng/ml). Changes of both NO and sLOX-1 in all acute stroke patients are showed in Figure 1. Figure1. Changes of NO and sLOX-1 in all acute stroke patients compared with the control. *, P<0.05 References 1. Castillo J, Rama R and Dávalos A. Nitric Oxide–Related Brain Damage in Acute Ischemic Stroke. Stroke,2000, 31, 852-857 2. Cano C. et al. Increased Serum Malondialdehyde and Decreased Nitric Oxide within 24 hours of Thrombotic Stroke Onset. Am J Ther 2003, 10(6),473-476. 3. Chatchanayeunyong R. and Suwanprasert K. Vascular Oxidative Stress through Superoxide Dismutase (SOD) and Intracellular Reactive Oxygen Species activated by ox LDL mediated LOX-1 receptor expression. Thammasat Medical Journal 2009, 9(2), 164-173. 4. Schwarz DA. et al. Identification of Differentially Expressed Genes Induced by Transient Ischemic Stroke. Molecular Brain Research 2002, 101, 12-22. 5. Murase T et al. Identification of Soluble Forms of LOX-1. Arterioscler Thromb Vasc Biol, 2000, 20, 715-720