Download
1 / 34
781 likes | 3.33k Views
Iron Deficiency Anemia. Prof.Dr .Teoman SOYSAL. Iron Deficiency Anemia. One of the most common medical problems Most common cause of anemia Iron deficiency anemia is the last step ; Iron depletion : absent or decreased iron stores

E N D
Iron Deficiency Anemia Prof.Dr.Teoman SOYSAL
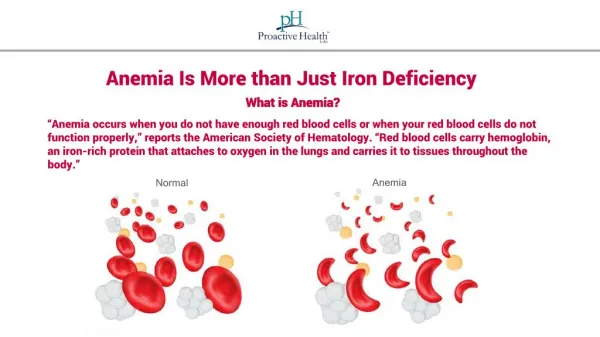
Iron Deficiency Anemia • One of themostcommonmedicalproblems • Mostcommoncause of anemia • Irondeficiencyanemia is thelast step ; • Irondepletion: absentordecreasedironstores • Irondeficiency: depletion of stores + low serum ironandferritin • Irondeficiencyanemia: Anemiadeveloping in an irondeficientpatient
IronMetabolism • Iron is located at thecenter of Hem molecules of Hb (amount:1.5-2 gr) and it is also; • Part of themyoglobin • Takesplace in thetissueenzymes • Storageformsare(1gr in men,0.5gr in women): • Ferritin • Hemosiderin • Location: Bone Marrow, Liver, Spleen • Transport ironis about 7 mg andboundtotransferrin.
Iron Metabolism • Transferrinpicksupironfrom ; • The GI cellsto deliver it toHbformingcells • Storageparts as a step of ironrecyclingprocess • Absorbtion + recyclingprovidestheconstantironsupply of 20 mg/day(upto 35 mg)necessaryforHbsynthesis
Daily Iron Demands Male1 mg Adolesc. 2-3 mg Women in repr.age 2-3 mg Pregnant 3-4 mg
Iron Metabolism • Ironabsorbtion is restrictedtotheneeds of the body • 1mg of iron is losteachday • Sweating • Epidermalshedding • Menstruationandpregnancy/lactationareothermajorcauses of ironlossandincreseddemand in women
Iron Metabolism • Normal dietcontainsabout 15 mg of iron/day • 6mg elementaliron/1000 cal • 1/10 of ingestediron is absorbed • Gastricacidreleasesironfromfood • Iron is absorbed in thereduced form • Ascorbateincreasesabsorbtion (byreducing) • Phytates,tannates,antacidsdecreaseabsorbtionbymakingcomplexeswithiron
Iron Metabolism • Main sites of absorbtion are; • Duodenum • Upper jejunum • Malabsorbtive states or gastrojejunostomy prevent absorbtion.
Iron Metabolism Transport of iron • Transferrin is the main iron carrier in plasma • It is produced in liver cells with increased synthesis in iron deficiency • Transferrin binds 1-2 ferric iron molecules • Transferrin-iron complex is endocytosed by Hb producing cells after linking to receptors.
Iron Metabolism • Total iron binding capacity and iron • Transferrin is measured by quantifying the iron binding sites available • This is also called “Total iron binding capacity” • TIBC is 1/3 saturated under normal conditions • Plasma Transferrin : 300 μg/dL • Plasma Iron: 60-180 μg/dL
Causes of iron deficiency • Chronicbloodloss • Increaseddemand • Malabsorbtion of iron • Inadequateironintake • Intravascularhemolysisandhemoglobinuria-hemosiderinuria • Combinations
Increased demands • Pregnancy • Lactation • Rapid growth
Decreased intake • Decreased iron in the diet • Vegetarianism • Tea-tost type feeding (old age) • Decreased absorbtion • Gastric surgery • Achlorhydria • Sprue • Pica
Increased iron loss • Menorrhagia • GIS hemorrhagia • P.Ulcer • Oesophagitis • Varices • Hiatal hernia • Malignancy • Angiodysplasia • Diverticulosis • Meckel diverticula • Colitis or imf. Bovel disease • Hemorrhoids • NSAID use • Parasites
Increased iron loss • Bleedingdisorder • Pulmonarylesionswithbleeding • Hemoglobinuria – hemosiderinuria (chronicintravascularhemolysis) • Hemodialysis • Hematuria (chronic) • Frequentdonation • 250 mg iron /unit-blood
Clinical features • General symptoms of anemia • Fatiguemay be disproportionaltothedegree of anemiaduetodeficiency of tissueenzymeswhichalsoneediron • Chlorosis • Glossitis • Angularstomatitis • Paterson-Kelly (PlummerVinson) syndrome (oesephageal web leadingtodisphagia)
Clinicalfeatures • Gastric atrophy • Ozena-anosmia • Nail changes • Brittle/fragility • Koilonchia/spooning • Hair loss • Splenomegaly
Clinical features • Pica:Appetiteforbizzarefood/substances • Geophagy (earth,clay) • Pagophagia(ice) • Amylophagia(starch) • Developmentalproblems • Splenomegaly • Tayanc-Prasadsyndrome (growthretardation, hypogonadism, hepatosplenomegaly, zincandirondeficiency, geophagia) • Immun-deficiency
Lab. Features • Hb,Htc,RBC:Low • MCV,MCH,MCHC:Low • RDW: High • Retics: Normal/Low • Plt:Normal/Low/High • WBC:Normal/Low • Smear: Hypochromia,anisocytosis,microcytosis, poikilocytosis
Lab.Features • Serum Iron: (N: 60 – 180 μg/dL) • TIBC: (250 - 430 μg/dL) • Serum Ferritin (N:Female;10-150 μg/L, Male;29-248 μg/L) Malesandpost menopausalwomen<10 μg/L Premenopausalwomen <5 μg/L Iron def+Chr.Disease< 60 μg/L
Lab.Features • Transferrinsaturation (Fe/TIBC):(<15%)<5%:definitelyindicatesirondeficiency • Serum Transferrin Receptor: • FreeErythrocyteProtoporphyrin(17 – 27 μg/dL) • Bone marrow : • Erythroid hyperplasia, • Absence ofhemosiderin
Differential diagnosis • Microcyticanemias • Irondeficiencyanemia • Thalassemia ,HbC,HbEetc • Sideroblasticanemia • Leadpoisoning • Anemia of chronicdiseases (sometimes)
Diff.Diagnostic Tests Iron deficiency Chronic disease Siderobl.anemia Thalasse-mia. Lead poisoning aminolaevulinic acid porphobilinogen
Important !!!!!!! • The diagnostic procedure is not complete until the underlying pathology is disclosed.
Treatment • Replaceironandtreatunderlyingdisease. • Oral route is preferredforreplacement. • Response can be followedbyretic. increase in 1-2 weeks (5-7 days) • Hbresponsetotreatment • half normal by a month • returnsto normal by 2-4 months • Replacementtherapy is prolongedby 6-12 monthstoreplenishstores of iron. • Ongoingbleedingmaycauseindefinitetherapy.
Treatment Oral iron therapy: dose (mg) elemental iron(mg) Fe fumarate 200 65 Fe gluconate300 35 Fe sulphate 200 65
Treatment Oral iron therapy: Total daily dose:150-200 mg elemental iron Give in 3-4 divided doses, Each one hour before meals. Do not prefer enteric coated forms. In case of GIS intolerance; • Change the route of administration or • Change the preparation or • Reduce dose
Treatment Nonrespondingpatient: • possiblecauses • Misdiagnosis • Patientdoes not takethemedicine • Continuingbloodloss • Malabsorbtion • Changethedrug • Changetheroute of administration • Underlyingdisease /comorbidity • Combineddeficiency
Treatment • Parenteral iron therapy: Routine use is not justified, Response is not faster than oral replacement. Indications • Malabsorbtion • Intolerance to oral replacement • Colitis/enteritis • Needs in excess of amount that can be given orally • Patient uncooperative/poor compliance • Autologous blood donation setting • Hemodialysis
Treatment Parenteralirontherapy: Total irondose:(15-patientHb) x bw x 3 • IronDextran: 50 mg/ml (iv/im) • Maxdailydose is 100 mg im • Ferricgluconate: • A test dose of 25 mg elementaliron (2 mL) must be given in 50 mL salineover 60 minutes • Ferric-hydroxy-sucrose(100 mg/5mL) • 2.5 ml firstday • 5ml thirdday • 2x5 ml/week
Parenteralreplacementtherapymaycause allergicreactions, localpainorinduration, serum sicknesslikedisease, lymphadenomegaly, arthralgia, myalgiaetc. Treatment
preventiveironsupplementation • Pregnants ( at 20-24 weeks Hb< 11 g/dL, Ferritin ). • Lactation. • Frequent blood donation. • Autologous blood donation settings. • Gastrectomised patients. • High dose asprin treatment.