Download
1 / 33
330 likes | 471 Views
Anti-Mullerian Hormone in the pathophysiology of PCOS. Roy Homburg Homerton University Hospital, London & Barzilai Medical Centre, Ashkelon, Israel. Anti-Müllerian hormone ( TGF- β superfamily: Müllerian duct regression in male embryos).

E N D
Anti-Mullerian Hormone in the pathophysiology of PCOS Roy Homburg Homerton University Hospital, London & Barzilai Medical Centre, Ashkelon, Israel.
Anti-Müllerian hormone(TGF-β superfamily: Müllerian duct regression in male embryos) Maximal expression occurs in preantral and small antral follicles1,2 Expression disappears in maturing pre-ovulatory follicles (expression restricted to GCs of the cumulus)2 1. Laven et al. J Clin Endocrinol Metab 2004; 89: 318–323; 2. Weenen et al. Mol Hum Reprod 2004;10: 77–83; 3. Cook et al. Fertil Steril 2000; 73: 859–861; 4. La Marca et al. Hum Reprod 2004; 19: 2738–2741; 5. La Marca et al. Hum Reprod 2006; 21: 3103–3107
AMH AMH is expressed in pre- antral and small antral follicles. AMH is thus a good indicator of the size of the ovarian antral follicle pool.
PCOS morphology x6 the density of pre-antral follicles compared with normal ovary. Webber et al, 2003 AMH serum concentrations in PCOS are high
PCOS PCOS – individual follicles produce more AMH Intrinsic property of PCOS granulosa cells or ? Due to A’s or insulin
Individual cell dysfunction in PCOS X 75 X 4-18 AMH concentrations in size-matched granulosa cells Anovulatory PCOS Ovulatory PCOS Normal ovaries (Pigny et al, 2003; Pellatt et al, 2007)
Antral follicle dysfunction- Arrest of growth/anovulation Dewailly et al, 2007 The size of the 2-5mm follicle pool is an independent and important contributor to the follicular arrest of PCOS.
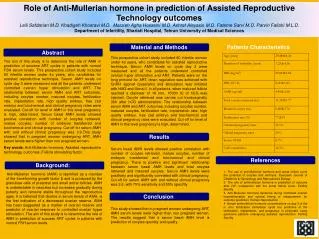
The relationship of serum anti-Mullerian hormone with polycystic ovarian morphology and polycystic ovary syndrome: A prospective cohort study. R. Homburg, A. Ray, P. Bhide, A. Gudi, A.Shah, P. Timms and K. Grayson Homerton University Hospital, London Hum Reprod, 2013
PCOS & AMH Pre- antral and small antral follicles produce AMH x6 the density of pre-antral follicles compared with the normal ovary in PCOS. (Webber et al, 2003) High AMH levels in PCOS also due to increased production by individual follicles (Pellatt et al, 2007) Some have suggested that asymptomatic polycystic morphology (PCOM) is not an entity but a mild variation of normal.
Study aims 1. To define the place of polycystic ovarian morphology (PCOM) in the hierarchy of polycystic ovary syndrome (PCOS). 2. To investigate the relationship of AMH to gonadotrophin concentrations. Homburg et al, Hum Reprod,2013
Homburg et al, Hum Reprod,2013 Data was collected prospectively from three groups of women before undergoing fertility treatment: PCOS (Rotterdam criteria) n=90 Polycystic ovarian morphology but no symptoms (PCOM) n=35 Normal ovaries – controls matched for age and BMI n=90
Matched for age and BMI Homburg et al, Hum Reprod,2013
AMH concentrations AMH measured by Beckman-Coulter Gen II assay
Mean values and 95% confidence intervals for AMH (pmol/l) in the group of controls (N), PCOM and PCOS.
Conclusion Serum AMH concentrations are capable of differentiating between normal ovaries, PCOM and PCOS. Suggests that the number of small follicles determines the severity of the syndrome. Homburg et al, Hum Reprod,2013
AMH levels in PCOS according to the menstrual status Menstrual status Regular cycles Oligomen-orrhea Amenorrhe AMH (pmol/L) 58.4 (31.9) 83.6 (60.3) 120.4 (50.8) Number of patients 18 44 9 Pignyet al., 2006 Higher AMH values in oligo - amenorrheic women and in women with hyperandrogenism
Kolhapur PCOS study – ‘MAPIN’ study 2007 – 2011 1257 women with PCOS – Rotterdam Criteria Analysis ready for 492 Clinical Endocrinology and Metabolism Ultrasound (Kulkarni, Gudi, Homburg and Conway)
Kolhapur PCOS study – BMI quintiles (Kulkarni, Gudi, Homburg and Conway)
Kolhapur PCOS study – hirsutism F-G Score
Effect of aging on PCOS Women with PCOS gain regular menstrual cycles when aging Menstrual cycle restored in those with a smaller follicle count Elting et al, 2000, 2003
Lack of influence of endogenous FSH FSH levels generally lower than normal but within normal limits. Adding exogenous FSH (CC, low dose FSH) restores normal follicular growth. Increased responsiveness to exogenous FSH Suggests an endogenous inhibition of FSH action in PCOS.
Mean values and 95% confidence intervals for FSH (IU) in the groups of control (N), PCOM and PCOS.
Possible role of AMH in the pathophysiology of PCOS • The size of the 2-5mm follicle pool is an independent and important contributor to the follicular arrest of PCOS. (Dewailly et al, 2007) • AMH concentrations are very high in PCOS. The higher they are, the greater the ovulatory disturbance. (Pigny et al, 2006) • Action of FSH in promoting follicular growth is counteracted by AMH. (Pigny et al, 2003;Weenen et al, 2004; Durlinger et al, 2001)
Anovulation A excess LH +insulin Multiple small follicles AMH FSH action Anovulation progesterone
Treatment • Weight loss – Lower AMH at start do better if AMH falls ovulation (Moran et al, 2007) • CC in obese & laparoscopic ovarian drilling – Response dependent on initial AMH conc. (Amer et al, 2009) • Metformin– Very long time for AMH to fall (Fleming et al, 2005) • FSH – AMH falls with Rx (Catteau-Jonnard, 2007)
Conclusions The severity of symptoms of PCOS is positively related to the number of small follicles reflected by AMH. AMH may play an important part in the pathophysiology of PCOS.