Download
1 / 21
210 likes | 242 Views
Antimicrobial Agents (Sulfonamides and Quinolones). Prof. R. K. Dixit Pharmacology and Therapeutics K.G.M.U. Lucknow dixitkumarrakesh@gmail.com. Objectives. After completion of this lecture you will be able to Know about sulphonamides Types (Classification) MOA

E N D
Antimicrobial Agents (Sulfonamides and Quinolones) Prof. R. K. Dixit Pharmacology and Therapeutics K.G.M.U. Lucknow dixitkumarrakesh@gmail.com
Objectives After completion of this lecture you will be able to • Know about sulphonamides • Types (Classification) • MOA • Combination with Trimethoprim or Pyrimethamine • Uses • ADRs, DDI, and Contraindications • Special points • Know about Quinolones • Types (Classification) • MOA • Uses • ADRs, DDI, and Contraindications • Special points
Quinolones and Fluoroquinolones • Have Quinolone structure • Nalidixic acid is first member • Fluorination of Quinolones - Fluoroquinolones • Gram negative mainly • (Plus gram positive New FQs) • N to P
MOA- (Queen stops gyrating dancers) • In gram negative – • Inhibition of DNA gyrase enzyme (Inhibit negative super coiling) • In gram positive – • Inhibition of Topoiosmerase IV – Inhibition of nicking and separation of daughter DNA strands after DNA replication (Inhibition of Decatenation) • The malformed DNA is digested by Exonucleases • Why not human cells affected ? • Mammalian cells have Topoiosmerase II
Resistance- • Due to mutation in chromosomes • Altered DNA gyrase and Topoisomerase IV • Reduced permeability for drug • Increased efflux of drug
Members Fluoroquinolones • First Generation • Ciprofloxacin • Norfloxacin • Pefloxacin • Ofloxacin Quinolones • Nalidixic acid Fluoroquinolones New Generations • Lomefloxacin • Levofloxacin • Prulifoxacin • Sparfloxacin • Gatifloxacin • Gemifloxacin • Moxifloxacin • Trovafloxacin • Alatrofloxacin • Finafloxacin Second Third Fourth MAN Can SPOT Good Life
M A N Can S P O T Good Life • Moxifloxacin • Alatrofloxacin • Norfloxacin • Ciprofloxacin • Sparfloxacin • Pefloxacin • Prulifoxacin • Ofloxacin • Trovafloxacin • Gatifloxacin • Gemifloxacin • Lomefloxacin • Levofloxacin
Nalidixic Acid- • Gram negative, (Narrow spectrum) • Bactericidal, • Acts by DNA gyrase inhibition, • Highly protein bound, • High concentration is inUrine • Neurological toxicity(vertigo, visual and seizures) • Haemolysis in G-6PD deficiency • Used as • Urinary antiseptic, • Bacterial Diarrhea. • Don’t give with Nitrofurantoin (Antagonism)
First generation FQs • Ciprofloxacin- • Long Post Antibiotic Effect (PAE) • Less active at acidic pH • Interacts with food and calcium • High tissue penetrability ( Except BBB) • High conc. in urine and bile • CNS side effects are common, • Tendonitis and tendon rupture • Drug Interaction- • Inhibition of metabolism of other drug, • Chelation • QT interval prolongation
USES- (Extended spectrum) • CNSI, MFI, OI, ENTI, RTI, GITI, UTI, PID, STDs, SBI • Nosocomial Infections • Septicaemia • Tuberculosis- MDR TB and XDR TB • Typhoid • Treatment 2 weeks • Prevention of carrier state 2 months • Other drugs- • Other FQs • Cephalosporins ,Ceftriaxone (Fastest) • Chloramphenicol • Cotrimoxazole • Ampicillin
Norfloxacin – • Less potent, • Primarily used for UTI and GIT infections, • Ofloxacin- • Highly active against Mycobacterium leprae • Pefloxacin – • Methylated derivative of Norfloxacin, • Oral bioavailability is 100%
Second Generation FQs • Lomefloxacin – • Once a day dose • Levofloxacin – • Levo-isomer of Ofloxacin, • Oral absorption is 100% • Single daily dose • Minimal drug interactions
Sparfloxacin – • Enhanced action against Chlamydia, • Maximum half life and Plasma Protein Binding • Second line Anti-tubercular drug • MAC in AIDS, Leprosy • No interaction with Theophylline and Warfarin, • Photoxicity • Single daily dose, • May prolong Q-T interval ( Avoid with Cisapride, TCAs, Phenothiazines, Anti-arrhythemics, Hypokalemia)
Gatifloxacin – • Prolongs Q-T interval, • Unexpected Hypo or Hyperglycemia in Diabetes mellitus patients. ( Withdrawn ) • Moxifloxacin – • Most potent FQ against M. tuberculosis. • Can prolong Q-T interval, • Phototoxic • Trovafloxacin – • Hepatotoxic (Reserved and maximum of 15 days Tt.) • Alatrofloxacin - Prodrug of Trovafloxacin • Finafloxacin, Prulifoxacin, Gemifloxacin
Elimination of Fluoroquinolones • Renal • Norfloxacin • Ofloxacin • Ciprofloxacin • Lomefloxacin • Levofloxacin • Gatifloxacin • Hepatic • Pefloxacin • Moxifloxacin • Trovafloxacin • Sparfloxacin • Gemifloxacin Fluoroquinolones safe in renal failure PefloxacinMoxifloxacinTrovafloxacin
Miscellaneous points about Quinolones • No FQs effective against spirochaetes • Ofloxacin and Pefloxacin are effective against M. leprae • Moxifloxacin is the only FQ NOT used in UTI as its concentration is poor in urine
Levofloxacin, Moxifloxacin, Gemifloxacin, Gatifloxacin, Sparfloxacin have good activity against S. pneumonia and also called Respiratory FQs. They also have good activity against anaerobes • Chronic Prostatitis Tt. Ciprofloxacin for 1 to 2 months • Gonorrhea- Tt. Single dose Ciprofloxacin 500mg • Chlamydia trachomatis- Ciprofloxacin one week or single dose Azithromycin
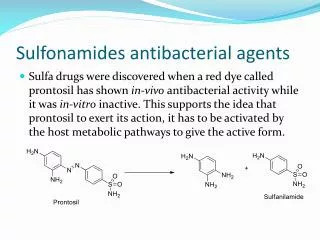
Summary • Sulphonamides • Act by inhibition of folic acid synthesis • Combined with Trimethoprim • Produce Stevens Johnson Syndrome • Prolonged use may produce hypothyroidism, goitre, arthritis and drug fever • Quinolones • Act by inhibition of DNA gyrase or Topoiosmerase IV • Have extended spectrum • Have chelating and enzyme inhibition property • Used for multiple infective diseases