Download
1 / 19
190 likes | 382 Views
Incidence of Leakage. Fielding 1980 Multi-centre prospective audit of 1466 colorectal anastomoses Leak Rate Intraperitoneal 10.8% Pelvic 18.7% Overall 13%. Trent/Wales and Wessex Audits. Incidence of Leakage. Incidence of Leakage. ACPGBI Guidelines: 2001

E N D
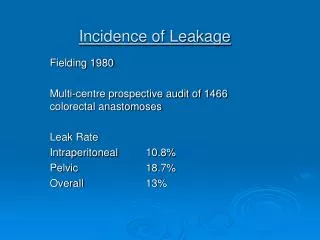
Incidence of Leakage Fielding 1980 Multi-centre prospective audit of 1466 colorectal anastomoses Leak Rate Intraperitoneal 10.8% Pelvic 18.7% Overall 13%
Trent/Wales and Wessex Audits Incidence of Leakage
Incidence of Leakage ACPGBI Guidelines: 2001 “Surgeons should carefully audit their leak rates for colorectal surgery and should expect to achieve an overall leak rate of below 8% for anterior resection and 4% for other colonic anastomoses.”
Incidence of Leakage Why has the incidence of leakage gone down? Widespread use of stapling guns. Increased sub-specialisation. ?Better patient selection. Widespread use of audit
Cause of Leaks Technical - Construction - Vascularity Failure to Heal - Hypoxia - Hypo-perfusion - Co-morbidity
Vascularity of Left Colonic Pedicle JD Griffiths: Arris & Gale lecture 1956 “A truly critical point exists at the splenic flexure where the marginal artery is often small --- the terminal branches of the left colonic artery form a secondary marginal artery at this point.”
Co-morbidity & Anastomotic Leak • Ischaemic heart disease • Acute and chronic respiratory disease • Diabetes • Old age • Co-existing sepsis • Previous radiotherapy • Smoking.
What do I do? Anastomotic Levels High Low Ultra low
What do I do? Options • Anastomosis alone • Anastomosis with proximal stoma • End colostomy with closed rectal stump (Hartmann’s procedure) • End colostomy with full ano-rectal excision (abdomino-perineal excision)
What does a proximal stoma achieve? It does: - reduce the number of clinical leaks. - reduce the need for further surgery in the event of a leak. It does not: - prevent breakdown of a poorly constructed or poorly perfused anastomosis. - provide a guarantee against major sepsis.
Complications of Ileostomy Formation and Closure
What do I do? No Anastomosis • Dubious blood supply to left colonic pedicle • Major co-morbidity • Pre-existing pelvic sepsis • Residual pelvic tumour
What do I do? High Rectal Anastomosis
What do I do? Low Rectal Anastomosis
What do I do? Ultra L ow Anastomosis