Download
1 / 15
150 likes | 265 Views
The Role of Anticoagulants. Keith A A Fox Edinburgh Centre for Cardiovascular Science. Disclosure Statement Keith A. A. Fox. President of the British Cardiovascular Society 2009-2012 European Society of Cardiology: ESC Programme Chair 2012-2014 KAA Fox member of the ESC guidelines group:

E N D
The Role of Anticoagulants Keith A A Fox Edinburgh Centre for Cardiovascular Science
Disclosure StatementKeith A. A. Fox • President of the British Cardiovascular Society 2009-2012 • European Society of Cardiology: ESC Programme Chair 2012-2014 • KAA Fox member of the ESC guidelines group: • ESC Guidelines: Non-ST elevation ACS EHJ (2007) 28, 1598–1660 • ESC Guidelines: ST Elevation MI EHJ (2008) 29: 2909-2945 • Co-Chair ROCKET-AF, Steering Committee • Major funding: British Heart Foundation, Medical Research Council and the Wellcome Trust • Additional funding: Bayer, Janssen, Sanofi, Lilly, Astra Zeneca • No stock ownership
Untreated and Under-treated Patients • Clear need to: • Identify patients with unsuspected AF and stroke risk • Anticoagulate those at stroke risk • Improve adherence to anticoagulation • Aspirin is not an adequate therapy for stroke prevention in AF
Lowest Effective Intensity for WarfarinTherapy 15 INR Odds Ratio 2.0 1.0 1.7 2.0 1.5 3.3 1.3 6.0 10 Odds Ratio 5 3 1 1.0 1.5 2.0 3.0 4.0 7.0 INR • INR below 2.0 results in a higher risk of stroke Hylek EM, et al. An analysis of the lowest effective intensity of prophylactic anticoagulation for patients with non-rheumatic atrial fibrillation. N Engl J Med. 1996;335:540-546.
Risk of Intracranial Haemorrhage(Outpatients) • PTR above 2.0 increases the risk of bleeding • The odds ratio of subdural hemorrhage increased 7.6 fold as the PTR increased from 2.0 to 2.5 18.2 11.2 10 8 6 Odds Ratio 4 2 0 0 1.4 1.6 1.8 2 2.3 2.7 Prothrombin Time Ratio Hylek EM, and Singer DE. Risk factors for intracranial hemorrhage in outpatients taking warfarin. Ann Intern Med. 1994;120:897-902.
Warfarin vsAntiplatelet Agents Systematic Overview 4.5 million people with AF in the EU Hart RG, et al. Ann Intern Med. 2007;146:857-867.
Problems With Vitamin K-Based Oral Anticoagulation • Risk of bleeding • Many contra-indications • Narrow therapeutic window • Frequent blood testing • Many drug interactions • Discontinuations for surgery/procedures • Lifestyle restrictions
Finding the right balance is key! Stroke and ACS Risk Bleeding Risk
The Dutch Bypass Oral Anticoagulants Study: Distribution of Time in Each INR Range 450 RANGE 400 50% 350 300 Time in INR Class (patient-years) 250 200 150 100 50 0 1 1.5 2 2.5 3 3.5 4 4.5 5 5.5 6 6.5 >6.5 INR Dutch bypass OA vs ASA. Lancet.2000;355:346-351.
Tolerability of Warfarin During First Year of TherapyElderly Patients in the US • 58% time in therapeutic range • Major haemorrhage 7.2%; ICH 2.5% • Rates were 2.75× higher in patients ≥80 years • 28% of patients discontinued warfarin at 1 year Hylek EM, et al. Circulation. 2007;115:2689-2696.
Time in Therapeutic Range (UK)n=2,074,928 INRs in Primary Care http://www.4s-dawn.com/products/anticoagulation/dawn-ac-benchmarking-service/
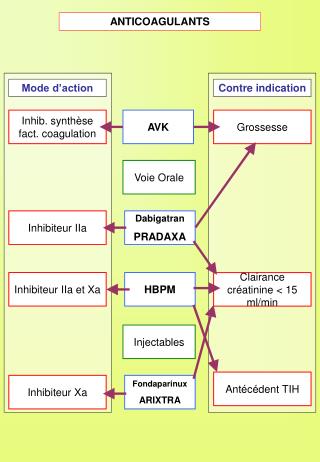
Targets for Anticoagulants ORAL DIRECT PARENTERAL INDIRECT TF/VIIa X IX IXa VIIIa Rivaroxaban Apixaban Edoxaban Va Fondaparinux Xa LMWH II UFH IIa Dabigatran AZD 0837 Fibrinogen Fibrin Weitz JI, Bates SM. J ThrombHaemost. 2005;3:1843-1853. Weitz JI, et al.Chest. 2008;133:234-256. 12
NOACs vsWarfarin: Trial Summary NB: trial populations differ in characteristics Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151.[1] Patel MR, et al. N Engl J Med. 2011;365:883-891.[2] Granger CB, et al. N Engl J Med. 2011;365:981-992.[3] GiuglianoRP, et al. N Engl J Med. 2013;369:2093-2104.[4] * Edoxaban is not yet approved for stroke prevention in AF patients. † ITT population at baseline
ESC 2012 Guidelines: All Novel OACs Preferred Over VKAs Based on Net Clinical Benefit *Class of recommendation; #Level of evidence Camm AJ, et al. Eur Heart J. 2012;33:2719-2747.
So, based on the evidence, what is the future….? • Systematic detection of AF and stroke risk • Improved patient education for compliance • Registry programmes and quality control • Reduced stroke risk, ICH and major complications with “NOACs” • No need to routinely monitor • Do we need antidotes? Yes, rarely • New indications – AF and ACS, post ACS • The NOACs will become the norm for anticoagulation