Download
1 / 26
270 likes | 326 Views
Explore the roles of Angiotensin peptides, ACE inhibitors, & more in the Renin-Angiotensin system. Learn about receptors, actions, and peptide functions in this comprehensive medical guide.

E N D
Peptides Autacoids Dr Mahmoud Khattab
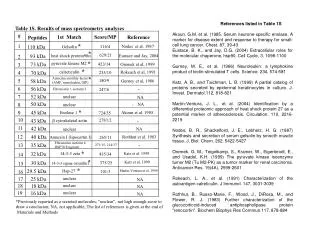
Angiotensins, Angiotensin II, and Blockers • The renin-angiotensin (Ang)-aldosterone system (RAAS) has vital pathophysiological & therapeutic importance • Angiotensins peptides derived from a high-molecular weight angiotensinogen, a plasma 2-globulin • Renin, released from the kidneys & others, converts angiotensinogen into a the decapeptide, angiotensin I (AngI, inactive) • Angiotensin-converting enzyme (ACE, peptidyly dipeptidase, kiniase), found in plasma & tissues including glands, kidneys, endothelium & heart
Renin Release • Renin releaseis stimulated by: • Β1-adrenergic stimulation • Decreased BP/Blood Volume, Renal Ischemia, Sodium Depletion • Drugs: ACEIs, ARBs Diuretics, Vasodilators • Renin releaseis inhibited by: NSAIDs, Β-adrenergic blockers
Angiotensins, Angiotensin II, and Blockers • ACEcleaves two carboxy terminal amino acids (9 and 10) of AngI to form the octapeptide AngII, the most active form • AngII is converted to a less active heptapeptide AngIII & other inactive fragments by a carboxy-peptidase • A new homolog of the enzyme, "ACE2" was identified • AngI/AngII are substrates for the enzyme, the products are the nonapeptide Ang-(1-9), or a heptapeptide Ang(1-7)
Metabolism of Angiotensin Peptides • Ang II can be converted to the heptapeptide Ang III by glutamylaminopeptidase or to ang (1-7) by prolylendopeptidase • Ang III generally is less potent than ang II but is equally potent as a stimulator of aldosterone secretion • Ang III can be metabolized to a hexapeptide (ang 3−8, ang IV) fragment by an arginylaminopeptidase • Ang IV is currently being studied as a biologically active peptide with potential physiologic significance
Angiotensin II Receptors • Two main receptors are identified: Type-1 & Type-2 angiotensin II receptors • Both are G-protein coupled receptors
Angiotensin II Type-1 Receptor Distribution & Function Physiologic functions of AT1 receptors according to their location
AT-1 Receptor-Mediated Actions of Angiotensin II • Vasculature: Vascular hypertrophy • Potent vasoconstriction of pre- & post-capillary blood vessels in skin, kidney & splanchnic areas (minor in brain & skeletal muscle) • Cardiac hypertrophy & fibrosis, positive inotropy • Increased NE release from sympathetic nerve terminals, adrenal medulla & brain (indirect vasoconstriction) • Aldosterone release from adrenal cortex • Antdiuretic hormone (ADH, vasopressin) release from pituitary gland
Paracrine Renal Effects of Angiotensin • AngI (AI) is generated in the afferent arteriole, converted to ang II (AII) by ACE • AII can cause mesangial cell contraction & efferent arteriolar constriction • AII can also be filtered at the glomerulus & subsequently act at the proximal tubular cells to increase sodium re-absorption • In the renal interstitium, renin produces angiotensin peptides that act at vascular and tubular structures • Angiotensin peptides may also be synthesized in and released from renal juxtaglomerular cells
AT-2 Receptor-Mediated Actions of Angiotensin II • Release of bradykinin • Production of nitric oxide, and increased cGMP • Vasodilation • Antiproliferative effect on vascular smooth and cardiac muscles • Stimulation of Apoptosis • Cell differentiation
Include atrial natriuretic peptide (ANP), brain natriuretic peptide (BNP), C-type natriuretic peptide (CNP) ANP derived from a 126 amino acids prohormone, secreted primarily from cardiac atria BNP, identified initially in brain, is secreted from both atria & ventricles CNP identified in brain & in vascular endothelial cells Stretch receptors in the atria and ventricles detect changes in cardiac chamber volume related to increased cardiac filling pressures, resulting in release of both ANP and BNP but not CNP The Natriuretic Peptide Family
The Natriuretic Peptide Family • The actions of the natriuretic peptides are mediated by natriuretic peptide receptors (NPRs),NPR-A/B/C • NPR-A & NPR-B are coupled to membrane-bound GC, increases levels of cGMP • NPRs are localized in vascular SM, endothelium, platelets, the adrenal glomerulosa, & the kidney • ANP & BNP increase urine volume & sodium excretion, decrease vascular resistance, and inhibit release of renin and secretion of aldosterone & vasopressin • Neutral endopeptidases (NEPs) inactivate NPs
Renin-Angiotensin-Aldosterone System (RAAS) Antagonists Angiotensin Converting Enzyme Inhibitors (ACEIs) • SH- compounds: captopril, zofenopril, pivalapril • Carboxyl compounds:benazepril, cilazapril, enalapril, lisinopril, perindopril, quinapril, ramipril • Phosphoryl compounds:fosinpril, ceronapril Mechanism & Site of Action: • Competitive inhibition of ACE, being structural analogs to the di-peptides cleaved by the enzyme • In exp animals & humans, they inhibit the pressor effect of IV angI denoting inhibition of conversion to angII • Inhibition of bradykinin degradation byACE leading to increased kinins levels (both therapeutic & side effect)
RAAS AntagonistsAngiotensin Converting Enzyme Inhibitors (ACEIs) Main Effects • Reduced formation of ang II leading to inhibition of most AT-1 receptor-mediated actions • Reduction of direct angII-induced vasoconstriction • Inhibition of angII-mediated sympathetic NS stimulation that might contribute to vasodilation • Significant reduction of plasma aldosterone levels leading to hyperkalemia & sodium depletion • Reduced vasopressin release→ increased water depletion (enhance diuretic effect)
RAAS AntagonistsAngiotensin Converting Enzyme Inhibitors (ACEIs) Main Effects • Increased levels of bradykinin → increased vasodilatation & induction of cough & itching • Increased plasma renin activity as a result of impaired angII-mediated feedback inhibition Therapeutic Uses & Adverse Effects Main uses are treatment of hypertension (HTN) & CHF, discussed later in respective lectures Detailed actions in HTN & CHF, and adverse effects, are to be discussed later with Prof Matrafi under respective topics
RAAS AntagonistsAngiotensin II Type-1 (AT-1) receptor Antagonists • They are competitive antagonists at AT-1 receptors with only low affinity to AT-2 R • They include drugs like losartan & valsartan • They block AT-1-mediated actions, similar to ACEIs but: • No effect on bradykinin, substance P, ACE • Feedback inhibition of angII is blocked→ ↑ renin release → increased angII Detailed actions in HTN & CHF, and adverse effects, are to be discussed later with Prof Matrafi under respective topics
RAAS AntagonistsVasopeptidase Inhibitors • Dual inhibitors of ACE & neutral endopeptidase • Examples: omapatrilat & ilepatril (Sanofi-Aventis Pharma) • They decrease circulating angIi and increase levels of ANP and bradykinin • They under clinical trials for treatment of hypertension, CHF, and diabetic nephropathy Renin Inhibitors • Enalkiren & ditekiren are inhibitors of renin • They lower BP hypertensive subjects • They are still investigated
Kinins • Bradykinin is an endogenous vasodilator nonapeptide, released from plasma α2-globulins kininogens • High molecular weight (HMW) form present in plasma & a low molecular weight (LMW) form present in tissues • Hydrolysis of plasma HMW kininogen, by plasma kallikrein, a protease, gives bradykinin
Kinins • Hydrolysis of LMW kininogen by tissue kallikrein →kallidin • Kallidin a vasodilator decapeptide with similar properties to those of bradykinin • Bradykinin is cataboloised by kiniase II, identical to peptidyl dipeptidase (ACE)
KininsReceptors, Actions & Therapy • The activate B1, B2, B3 receptors linked to PLC/A2 • Powerful Vasodilation→ decreased blood pressure via B2 receptor stimulation (NO-dependent) • Increase in capillary permeability inducing edema.It produces inflammation & algesia (B2) • Cardiac stimulation: Compensatory indirect & direct tachycardia & increase in cardiac output • It produces coronary vasodilation Bradykinin has a cardiac anti-ischemic effect, inhibited by B2 antagonists (NO & PI2 dependent)
KininsActions & Therapy • Kinins produce broncho-constriction & itching in respiratory system (antagonized by ASA) • Therapeutic Use: • No current use of kinin analogues • Increased bradykinin is possibly involved in the therapeutic efficiency & cough produced by ACEIs • Aprotinin (Trasylolol), a kallekrein inhibitor, used in treatment of acute pancreatitis, carcinoid syndrome & hyperfibrinolysis
Endothelins Vascular Endothelium ↓ Endothelium-Derived Contracting Factor (EDCF) (De Mey & Vanhoutte, 1982) ↓ Peptidergic EDCF (Hickey Et al., 1985) ↓ A 21-Amino Acid Peptide, Endothelin-1 (Yanagisawa et al., 1988
ETA Receptors Agonist: ET-1=ET-2>ET-3 Smooth muscles Actions: Contractile activity Vasopressor response Aldosterone release ETB Receptors Agonist: ET-1=ET-3 Smooth & endothelial cells Actions: Initial depressor effect Initial relaxant response Ex vivo platelet inhibition ETB receptors located on endothelium mediate NO- & PGI2-dependent vasodilatation Endothelin Receptors
Endothelin Therapeutic Potential • Endothelin-based therapy is Investigated for HTN, CHF • Bosentan is a dual ETA/ET B receptor antagonist • Receptor affinity ratio (ET A /ET B ) of 20:1, enhancing vasodilatory role in PAH by reducing ET A receptor activation • Bosentan reduces vascular remodeling • Adverse Effects: Elevated liver enzymes • headache (22%), nasopharyngitis (11%), flushing (9%), hepatic function abnormality (8%) and lower extremity oedema (8%)
Substance P • Substance P is an undecapeptide present in brain, afferent neurons, dorsal horn of spinal cord • It plays a role in pain transmission • It is present in intestine • It activates substance P GPCRs linked to EDHF • It produces vasodilation & contracts SM of GIT • MK-869 is a substance P antagonist tested for treatment of chemotherapy-induced emesis