Download
1 / 100
1k likes | 1.21k Views
Hematologic Disorders and Cancer. ACC Susan Beggs, RN MSN. Adult RBCs: 120 Lower H & H than child Lower WBCs than child . Pediatric RBCs: 100 days in neonate Increased erythropoiesis with age Higher H & H in children (17-18g) # of RBCs varies according to age.

E N D
Hematologic Disorders and Cancer ACC Susan Beggs, RN MSN
Adult RBCs: 120 Lower H & H than child Lower WBCs than child Pediatric RBCs: 100 days in neonate Increased erythropoiesis with age Higher H & H in children (17-18g) # of RBCs varies according to age Comparison of adult to pedi hematologic system
Risk factors associated with blood disorders in pediatric clients • More prone to anemia • Genetic characteristics may impair growth and development (sickle cell, hemophilia) • Immature immune systems to defend normal growth of cells • Higher risk of blood malignancies during childhood (ALL most common)
RBC Maturation • Basophilic erythroblast* • Orthochromic erythroblast* • Proerythroblast • Reticulocyte • Erythrocyte • Other cells that might be suggestive of disorders:
Components of the CBC • WBCs (leukocytes) • Neutrophils • Lymphocytes • Monocytes • Eosinophils • Basophils
Bands • Slighty smaller than other immature forms • Make up 0-6% of WBC count • Indicative of a shift to the left
Neutrophils • Segmented (segs) • Make up 45-75% of peripheral blood WBCs • Elevated indicative of a shift to the left or long term infection
What is peak and what is trough? • Peak refers to the effectiveness of the medication; checks saturation and penetration 30 min AFTER end of infusion • Trough check if too little or too much 30 minutes PRIOR to next dose
Iron deficiency anemia • Causes • Diagnostic tests to confirm • Treatments
Diagnostic tests to confirm IDA • hemoglobin • hematocrit, MCV • serum iron, RBC • Presence of reticulocytes (immature or newly released RBCs • Changes in iron-binding capacity • Serum ferritin < 15ng/ml
Treatments for IDA • Two major treatments: • Oral • Dietary teaching
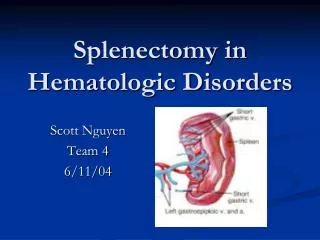
Types of sickle cell crisis • Vaso-occlusive • Aplastic crisis • Splenic sequestration crisis
Vaso-occlusive crises • Stasis of blood and clumping of cells in the microcirculation (capillaries) • May last from 1 day to several wks • Manifestations: • “What causes the pain?”
SCD, continued • Manifestations: • Chronic anemia (hgb 6-9) • Fatigue • Pain in areas of ischemia (joints) • Jaundice • Possible delayed sexual maturation • Susceptibility to sepsis • Possible growth retardation
What factors start the sickling? • Being submitted to hypoxia • Low blood pH (acidosis) • Increased blood viscosity • General stress • Infection
Aplastic crisis • Diminished RBC production • Results in severe anemia • Manifestations: • Headache • Pallor • Lethargy • **may be precipitated by infection
Splenic sequestration crisis • Sickled cells trapped in spleen • Blood flow is obstructed • Resulting in splenomegaly • May lead to : • Shock • Hypovolemia • tachycardia
Diagnostic Studies for SCD • Hemoglobin electrophoresis in NB • Child > 6 months of age, quick screen (Sickledex) • CBC results: • Decreased H & H (6-9 hgb) • Elevated reticulocytes (immature RBCs)
Nsg interventions for reactions to blood transfusions • Stay with patients the 1st 5-10 minutes after beginning the transfusion • STOP the blood if rx occur, but NOT the IV • Monitor VS • Listen for adventitious breath sounds that indicate overload
Insuring hydration in the child with SCD • Educating parents s/s dehydration • Instructions on # oz to replace fluids lost • Understand the “triggers” and precipitating factors • Monitoring I & O • Perform regular growth and nutritional assessments
Goals for SCD • Oxygenation • Adequate hydration • Pain relief • Prevention of infection • Education of child/family • No cure, but can be managed
Types and causes • Hemophilia A • Most common (75%) • Disorder with factor VIII • Bleeding most common symptom • Von Wildebrand is type of this hemophilia • Hemophilia B • Disorder with factor IX
Diagnostics and Treatment • Monitor studies which may be abnormal: PTT, Bleeding time, platelet counts, Factor VIII levels • Prevention and treatment of bleeding: • Protective gear for play • Limited activities • Replacement of clotting factors • Cold to cause vasoconstriction
Labs tests to confirm hemophilia • DNA testing for the trait • PTT prolonged • Bleeding time prolonged • Platelets and PT are normal • Low levels of factor VIII
Administering Meds for Hemophilia • Genetically engineered Factor VIII blood products; reconstituted with sterile water and given IV • Human plasma, fresh whole blood, fresh or frozen plasma (1 bag of concentrate per 5 kg of body weight is usually sufficient) • Vasopressin (DDAVP) IV
Nursing goals/interventions for the hemophiliac • Prevent bleeding or STOP bleeding • **Major cause of death: hemorrhage • Apply pressure 10-15 min • Elevate the joint above the heart • Immobilize the extremity • Apply cold compresses
“…communication promotes understanding and clarity; with understanding, fear diminishes; in the absence of fear, hope emerges; and in the presence of hope, anything is possible” (Stovall, 1995)
Causes of childhood cancers • Unlike adults, children don’t have the environmental exposures • May be genetic? • May be viral? Immune defects? • Genome project has identified genes for some of the cancers in children
Warning signs • C • H • I • L • D • R • E • N
Interventions for malignancies • Radiation • Chemotherapy (IV, po, intrathecal) • Surgery • Bone marrow and stem cell transplantation
Leukemias • Malignancies of the blood • Characterized by IMMATURE WBCs/blast cells • ALL most common (80%) • ANLL also common(20%)
Treatments for Leukemias • Staging must be done first to determine cell types • Remission induction • Possible CNS prophylactic therapy • Maintenance • Re-induction following relapse • BM transplantation • Prognosis
Chemotherapy protocol for leukemia Induction phase (hopeful remission) Consolidation phase Delayed intensification Maintenance phase 8/27/2014 50