Download
1 / 13
170 likes | 383 Views
Hospitalization-Associated Disability. Kenneth e. covinsky, md, mph; edgar pierluissi, md; c. bree johnston, md , mph. JAMA . 2011;306(16):1782-1793. Ryan Mullins MS-III Mercer University School of Medicine Dr. Rahimi- RTR Medical Group Savannah, GA 12/1/2011. Purpose of Discussion.

E N D
Hospitalization-Associated Disability Kenneth e. covinsky, md, mph; edgar pierluissi, md; c. bree johnston, md, mph. JAMA. 2011;306(16):1782-1793 Ryan Mullins MS-III Mercer University School of Medicine Dr. Rahimi- RTR Medical Group Savannah, GA 12/1/2011
Purpose of Discussion • In geriatric patients, acute medical illness requiring hospitalization often precipitates disability, resulting in an inability to live independently and complete basic activities of daily living(ADLs). • With an incidence of approximately 1/3 of hospitalized patients over the age of 70, hospitalization-associated disability(HAD) represents a problem that must be addressed. • This article presents a case of a 70 year old female who developed HAD and explores: risk factors and risk stratification tools that identify geriatric patients at increased risk of HAD; processes that may encourage HAD and models of care developed to prevent it; and methods clinicians can use to improve quality of life in geriatric patients who develop HAD.
Case • HPI: Ms. N is a 70 y.o. female who presented to the ED with left labial pain and hematuria for 3 days. • PMH: DMII, HTN, chronic kidney disease, CAD, PVD, and diabetic neuropathy. • SH: Ms. N emigrated from the Philippines in 1997. She was separated from her husband. Prior to admission, she lived independently in a friend’s home and was able to perform all of her ADLs until 3 days before admission. Her monthly income was $300/month from U.S. Social Security Administration. • PE: T: 98.2 BP: 155/42 mm Hg P: 55/min RR: 22/min Ms. N appeared frail and shivering. She had a tender, indurated 3 cm mass in the left labium majorum. She was AAO X3 and walked with a normal gait. • Lab studies: serum creatinine=10.8 mg/dL; K+=8.3 mEq/L; Hct=19.9%; albumin=3.2 g/dL.
Case Continued- Hospitalization Course • Day 1- Hemodialysis(HD) was started, and Ms. N received empirical treatment for a UTI. • Day 3- I&D of labial lesion. Ms. N was transferred to acute care for elders(ACE) unit. • While on ACE unit, Ms. N’s nurse noticed that Ms. N had myoclonus of her extremities, which resulted in difficulty of patient transferring from bed to commode. Mini-Cog screen at that time was negative. The ACE team discontinued Gabapentin at this time, which was started after admission for diabetic neuropathy. 5 days later, myoclonus had resolved, and Ms. N was again independent in ADLs and walking independently using a walker. • Ms. N continued having HD 3 times weekly. She was transferred from ACE unit to general medical ward while awaiting outpatient HD slot. • Over the next two weeks while on the general medical ward, Ms. N developed progressively worsening difficulty ambulating. Even using a walker, her gait was slow and unsteady. She began needing help using the commode and bathing. • Day 30- Ms. N was discharged to a skilled nursing facility.
HAD- Incidence • HAD- “loss of ability to complete 1 of the basic ADLs needed to live independently without assistance: bathing, dressing, rising from bed or a chair, using the toilet, eating, or walking across a room.” • HAD develops between the onset of the acute illness and d/c from hospital. • Of patients over the age of 70 hospitalized for a medical illness, at least 30% are discharged from the hospital with an ADL disability that they did not have prior to becoming acutely ill.1,2,3,4 • “Approximately 50% of disability among older adults occurs in the setting of medical hospitalization.”1,5 • One year post-discharge, less than 50% of geriatric patients have returned to baseline levels of functioning.1,6,7
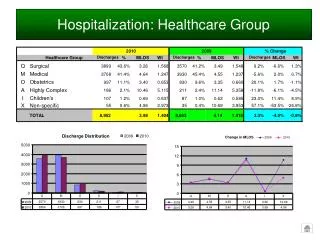
Incorporating Prevention of HAD Table 5. Processes of Hospitalization That May Lead to Hospitalization-Associated Disability and Quality Improvement Interventions From Acute Geriatric Units. Covinsky, K. E. et al. JAMA 2011;306:1782-1793
Effect of Disability After the Hospitalization • Whether a patient suffering from HAD will be able to live at home after being discharged depends on the patient’s capacity, social support, resources, and environment. • Planning a geriatric patient for discharge should include assessing ability to perform ADLs alone or with available assistance. • A home equipment evaluation for patients with new disabilities might be necessary to make sure patient’s home is safe (e.g.- stairs, showers, etc.). • Patient’s ability to understand medication instructions should be assessed.
Prognosis of HAD • “In a study of older adults who had developed hospitalization-associated disability, 41% died by 1 year, 29% remained disabled at 1 year, and only 30% returned to their preillness level of function.”1,6
References • Covinsky KE, Pierluissi E, Johnston CB. Hospitalization-Associated Disability. JAMA. 2011;306(16):1782-1793. • Covinsky KE, Palmer RM, Fortinsky RH, et al. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age. J Am Geriatr Soc. 2003;51(4):451–458. • Hirsch CH, Sommers L, Olsen A, Mullen L, Winograd CH. The natural history of functional morbidity in hospitalized older patients. J Am Geriatr Soc. 1990;38(12):1296–1303. • Gill TM, Allore HG, Gahbauer EA, Murphy TE. Change in disability after hospitalization or restricted activity in older persons. JAMA. 2010;304(17):1919–1928. • Gill TM, Allore HG, Holford TR, Guo Z. Hospitalization, restricted activity, and the development of disability among older persons. JAMA. 2004;292(17):2115–2124. • Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56(12):2171–2179. • Brown CJ, Roth DL, Allman RM, Sawyer P, Ritchie CS, Roseman JM. Trajectories of life-space mobility after hospitalization. Ann Intern Med. 2009;150(6):372–378.