Download
1 / 40
400 likes | 710 Views
Transplantation Science. Lars Wramner MD, Ph.D. Transplantation. Organs: Kidney, liver, heart, lung, pancreas Tissues: Cornea, skin, bone, heart valves Blood: Erythrocytes, trombocytes, plasma Bone marrow:. Transplantation. Autotransplantation Within one individual

E N D
Transplantation Science Lars Wramner MD, Ph.D.
Transplantation • Organs: • Kidney, liver, heart, lung, pancreas • Tissues: • Cornea, skin, bone, heart valves • Blood: • Erythrocytes, trombocytes, plasma • Bone marrow:
Transplantation • Autotransplantation • Within one individual • Isotransplantation • Between genetically identical individuals • Allotransplantation • Between individuals from the same species • Xenotransplantation • Between different species
Transplantation antigens • Antigen: A molecule recognised as foreign • Blood group antigens • The ABO-system • MHC: The Major Histocompatibility Complex • Humans: HLA, Human Leukocyte Antigens • Mouse: H2. Rats: RT1 • Enormous heterogeneity • Others
Specific -Nonspecific • Non -specific inflammatory mechanisms: • Macrophages, dendritic cells. • NK cells • Granulocytes • Complement • Antigen-specific immune response: • T-lymphocytes: TH, TC. • B-lymphocytes: Immunoglobulin, IG.
MHC • Location: • On the surface of nucleated cells. • Function: • Antigen presentation. A foreign molecule + the MHC-molecule = altered self => antigen. • Transplantation. A foreign MHC-molecule = altered self => transplantation antigen. • Inflammation: • Upregulated
Immune activation • Antigen presentation. • Cell-to-cell adhesion. • Signalling molecules. • Cytokine gene polymorphism. • Cell activation. • Effector mechanisms.
Antigen presentation • Antigen presenting cells, APC. • Macrophages, dendritic cells • Antigen presentation • Direct: Donor-APC with donor-MHC. • Indirect: Recipient-APC with donor-MHC.
Cell-to-cell adhesion • Close and stable adhesion: • Antigen presentation. • Facilitate signalling. • Adhesion molecules: • IgSF (ICAM, VCAM, LFA-3) • Integrins: 1,2,3, LFA-1 • Selectins: E,L,P-selectins
Signalling molecules • Co-stimulation • Cytokines: • Interleukins, IL • Interferons • TNF • TGF- • Others • Regulation of the immune response
Cytokine gene polymorphism • SNP, single nucleotide polymorphism. • Promoter region. • Detected by PCR-technique. • Inter-individual variation in cytokine- production or receptor activity. • Different clinical outcome.
Cell activation • Step 1: Antigen - cytokine • Ca-dependent pathway • Ca-independent pathway • Step 2: Cytokine - cell proliferation cycle • RAFT 1 • G1 -> S phase • Purine synthesis • DeNovo pathway • 7-10 days.
Effector mechanisms • TC (CD-8): Killer cells, cytotoxic cells. • TH (CD-4): Helper cells, promote inflammation. • B-lymphocytes: Antibody production,
Acute rejection • Cellular infiltration • Cytokine production • Upregulation of MHC • Tissue destruction • Cytotoxic T cells • Complement activation by antibodies • Thrombosis • Fibrosis
Clinical signs of acute rejection • Kidney: • Creatinine elevation • Lack of creatinine decline • Liver: • Abnormal liver values. • Thoracic organs • Protocol biopsies.
Clinical classification of rejections:- Chronological • Hyperacute: • Preformed antibodies. • Within minutes-hours. • Acute: • Mainly cellular • Within weeks, < 3 months. • Chronic: • After years, slowly progressing.
Clinical classification of rejections:- Sensitive to treatment • Steroid treatment: • Sensitive. • Resistant. Need for antibody treatment. • Outcome • Return to baseline level • Stable at an elevated level • Progressive
Chronic rejection • Inflammation • Arteriosclerosis • Intimal thickening • Fibrosis • Organ specific destruction's • Glomerular sclerosis and tubular atrophy • Vanishing bile ducts and cellular ballooning • Brochiolitis obliterans
Tolerance • Absence of activation: • Self tolerance! • Foetal tolerance! • Tumour tolerance? • Transplantation tolerance? • Mechanisms: • Anergy • Clonal deletion • Suppresser cells
Clinical results, kidney • Acute rejection: • 50 %. Nearly always reversible. • Increased risk of chronic rejection. • 1-year results: • 95 % patient survival. • 85-90 % graft survival. • Few infections, normal life. • Long term: • 50 % graft survival, appr 15 years.
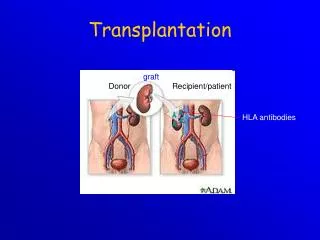
Val av främmande organ • Blodgruppstillhörighet. • Undantag, A2 -> 0 • Transplantationsantigen • Enäggstvilling • HLA-identiska syskon • Övriga utan främmande HLA-antigen • Med påvisbara främmande antigen, > 90 %
Historik • 60-talet: • Steroider (Prednisolon) • Azathiprin (Imurel) • 80-talet: • Calcineurinhämning I: Cyclosporin (Sandimmun) • Lymfocytantikroppar: Polyklonalt (ATG), monoklonalt (OKT-3) • 90-talet: • Calcineurinhämning II: FK506 (Prograf) • Purinesynteshämning: MMF (Cellcept) • TOR-hämning: Rapamycin (Rapamune), Everolimus (?) • IL-2 receptor hämning: Monoklonal a-k (Simulect, Zenapax)
Steroider • Verkan: Hämmar arachidonsyre kaskaden, antigenpresentation, cytokinproduction, adhesionsmolekyler och MHC-II och cellinteraktioner. • Biverkan: Hypertoni, blodsockerhöjning, osteoporos, acne, hudatrofi, hämmad sårläkning, ulcus och muskelatrofi. • Användning: • Profylax: Snabbt sjunkande, lågdos. • Rejektion: Högdos några dar.
Cytokinhämning I • Verkan:Synteshämning genom calcineurinblockad. • Cyclosporin, CyA: Sandimmun Neoral • Tacrolimus, FK506: Prograf • Biverkan: • Njurtoxicitet, hypertoni, hårväxt (CyA), tremor, gingiva hyperplasi, atheroscleros?
Cytokinhämning II • Verkan: Il-2 receptorblockad. Monoklonal antikropp, Simulect och Zenapax. • Biverkan: Immunhämning !? • Ges som injektion 2-5 gånger. • Immunhämning i 2-5 månader.
Cytokinhämning III • Verkan: Hämmar effekten av receptoraktivering genom blockad av TOR. • Rapamycin: Rapamune • Everolimus: ? • Biverkan: Hyperlipidemi, lätt benmärgshämning, ledbesvär, slemhinnesår, pneumonit. • Ej nephrotoxiskt. • Hämmar cellproliferation: Tumörer, blodkärlsendotel, ospecifik inflammation !? • Leflunomid ??
Hämning av celldelning • Verkan: Hämmar celldelning, främst lymfocyter, genom purinsyntes hämning. • Azathioprine (Imurel) • MMF (Cellcept). Mer selektivt för lymfocyter. • Biverkan: Buksmärtor och diarré, pancytopeni och slemhinnebesvär. • Mizoribine ? • Brequinarsodium ?
Antilymfocytantikroppar • Verkan: Något oklar. Förmodligen celldöd, lys, och redistribution. Ger långvarig lymfopeni i perifert blod. • Biverkan: • Kraftiga akut influensaliknande besvär. • Ledvärk. • Ökad infektionsrisk. • Risk för lymfom, senare. • Användning: • Induktion. • Avstötning. • Preparat: • Polyklonalt: ATG • Monoklonalt: OKT-3
Klinisk immunhämning I. • Inga mätmetoder av immunologisk hämning. • Läkemedelskoncentration. • Leukocytnivåer. • Allmänna doseringar: • Vetenskap, kliniska studier. • Beprövad erfarenhet. • Minimera biverkningar. • Kostnadseffektivt
Klinisk immunhämning II • Kombinationsterapi: • Trippel-, dubbel- eller monoterapi. • Successiv dosreduktion. • Profylaktisk terapi. • Induktion, högdos. • Underhåll, lågdos. • Avstötningsterapi: • Högdos steroider, 3-5 dar. • Antilymfocytantikroppar