Download
1 / 1
10 likes | 163 Views
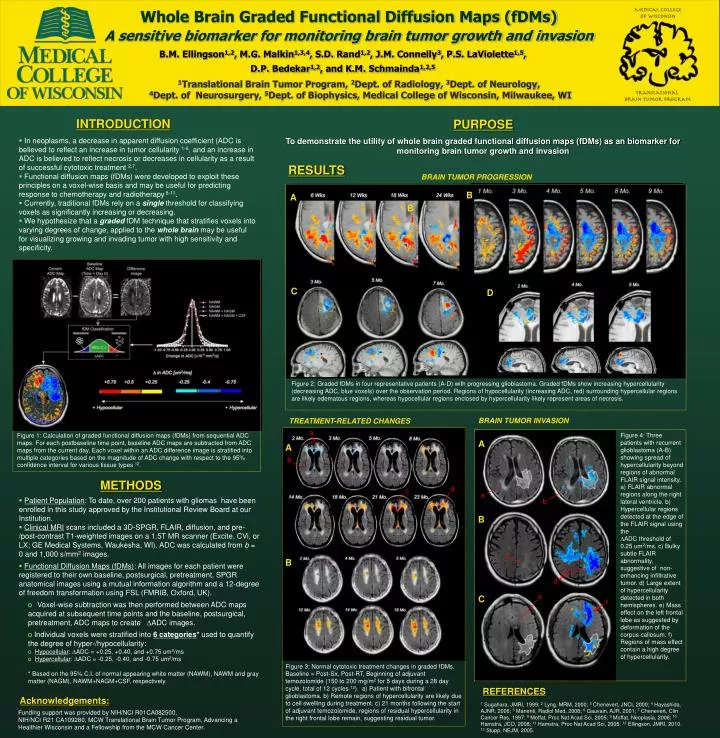
Whole Brain Graded Functional Diffusion Maps (fDMs) A sensitive biomarker for monitoring brain tumor growth and invasion.

E N D
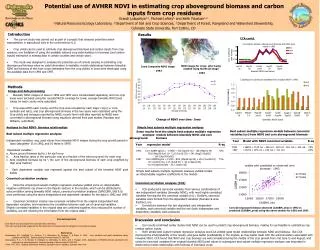
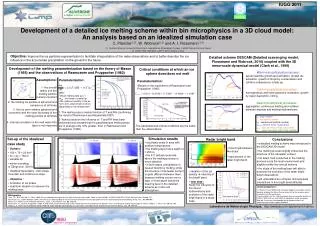
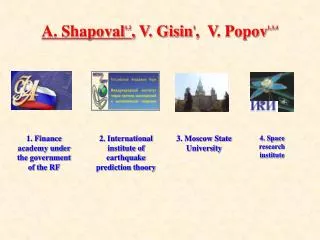
Whole Brain Graded Functional Diffusion Maps (fDMs) A sensitive biomarker for monitoring brain tumor growth and invasion Figure 1: Calculation of graded functional diffusion maps (fDMs) from sequential ADC maps. For each postbaseline time point, baseline ADC maps are subtracted from ADC maps from the current day. Each voxel within an ADC difference image is stratified into multiple categories based on the magnitude of ADC change with respect to the 95% confidence interval for various tissue types 12. B.M. Ellingson1,2, M.G. Malkin1,3,4, S.D. Rand1,2, J.M. Connelly3, P.S. LaViolette1,5, D.P. Bedekar1,2, and K.M. Schmainda1,2,5 1Translational Brain Tumor Program, 2Dept. of Radiology, 3Dept. of Neurology, 4Dept. of Neurosurgery, 5Dept. of Biophysics, Medical College of Wisconsin, Milwaukee, WI INTRODUCTION PURPOSE • In neoplasms, a decrease in apparent diffusion coefficient (ADC is believed to reflect an increase in tumor cellularity 1-6, and an increase in ADC is believed to reflect necrosis or decreases in cellularity as a result of successful cytotoxic treatment 2,7. • Functional diffusion maps (fDMs) were developed to exploit these principles on a voxel-wise basis and may be useful for predicting response to chemotherapy and radiotherapy 8-11. • Currently, traditional fDMs rely on a single threshold for classifying voxels as significantly increasing or decreasing. • We hypothesize that a graded fDM technique that stratifies voxels into varying degrees of change, applied to the whole brain may be useful for visualizing growing and invading tumor with high sensitivity and specificity. To demonstrate the utility of whole brain graded functional diffusion maps (fDMs) as an biomarker for monitoring brain tumor growth and invasion RESULTS BRAIN TUMOR PROGRESSION B A B C D Figure 2: Graded fDMs in four representative patients (A-D) with progressing glioblastoma. Graded fDMs show increasing hypercellularity (decreasing ADC, blue voxels) over the observation period. Regions of hypocellularity (increasing ADC, red) surrounding hypercellular regions are likely edematous regions, whereas hypocellular regions enclosed by hypercellularity likely represent areas of necrosis. BRAIN TUMOR INVASION TREATMENT-RELATED CHANGES a Figure 4: Three patients with recurrent glioblastoma (A-B) showing spread of hypercellularity beyond regions of abnormal FLAIR signal intensity. a) FLAIR abnormal regions along the right lateral ventricle. b) Hypercellular regions detected at the edge of the FLAIR signal using the ADC threshold of 0.25 um2/ms. c) Bulky subtle FLAIR abnormality, suggestive of non-enhancing infiltrative tumor. d) Large extent of hypercellularity detected in both hemispheres. e) Mass effect on the left frontal lobe as suggested by deformation of the corpus callosum. f) Regions of mass effect contain a high degree of hypercellularity. A A b METHODS d c a • Patient Population: To date, over 200 patients with gliomas have been enrolled in this study approved by the Institutional Review Board at our Institution. • Clinical MRI scans included a 3D-SPGR, FLAIR, diffusion, and pre-/post-contrast T1-weighted images on a 1.5T MR scanner (Excite, CVi, or LX; GE Medical Systems, Waukesha, WI). ADC was calculated from b = 0 and 1,000 s/mm2 images. • Functional Diffusion Maps (fDMs): All images for each patient were registered to their own baseline, postsurgical, pretreatment, SPGR anatomical images using a mutual information algorithm and a 12-degree of freedom transformation using FSL (FMRIB, Oxford, UK). • Voxel-wise subtraction was then performed between ADC maps acquired at subsequent time points and the baseline, postsurgical, pretreatment, ADC maps to create ADC images. • Individual voxels were stratified into 6 categories* used to quantify the degree of hyper-/hypocellularity: • Hypocellular: ADC = +0.25, +0.40, and +0.75 um2/ms • Hypercellular: ADC = -0.25, -0.40, and -0.75 um2/ms • * Based on the 95% C.I. of normal appearing white matter (NAWM), NAWM and gray matter (NAGM), NAWM+NAGM+CSF, respectively. b B c B d e C f Figure 3: Normal cytotoxic treatment changes in graded fDMs. Baseline = Post-Sx, Post-RT, Beginning of adjuvant temozolomide (150 to 200 mg/m2 for 5 days during a 28 day cycle, total of 12 cycles 13). a) Patient with bifrontal glioblastoma. b) Remote regions of hypercellularity are likely due to cell swelling during treatment. c) 21 months following the start of adjuvant temozolomide, regions of residual hypercellularity in the right frontal lobe remain, suggesting residual tumor. REFERENCES Acknowledgements: 1 Sugahara, JMRI, 1999; 2 Lyng, MRM, 2000; 3 Chenevert, JNCI, 2000; 4 Hayashida, AJNR, 2006; 5 Manenti, Radiol Med, 2008; 6 Gauvain, AJR, 2001; 7 Chenevert, Clin Cancer Res, 1997; 8 Moffat, Proc Nat Acad Sci, 2005; 9 Moffat, Neoplasia, 2006; 10 Hamstra, JCO, 2008; 11 Hamstra, Proc Nat Acad Sci, 2005. 12 Ellingson, JMRI, 2010. 13 Stupp, NEJM, 2005. Funding support was provided by NIH/NCI R01CA082500, NIH/NCI R21 CA109280, MCW Translational Brain Tumor Program, Advancing a Healthier Wisconsin and a Fellowship from the MCW Cancer Center.