Download
1 / 14
140 likes | 317 Views
Dyspnea and Rash. Andres Quiceno, MD Rheumatology PHD. Case. 42 y/o AAF CC : Dry cough and dyspnea for 2.5 months.

E N D
Dyspnea and Rash Andres Quiceno, MD Rheumatology PHD
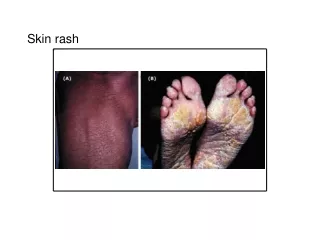
Case • 42 y/o AAF • CC: Dry cough and dyspnea for 2.5 months. • HPI: Patient started with dyspnea on exertion that progressed over 10 weeks to dyspnea at rest, accompanied by a dry cough. Two weeks prior to admission, the patient developed arthralgias in her ankles, knees, wrists and elbows with arthritis in her MTPS and PIPS. She also noticed rash on her knees, shoulders and neck, described as erythematous with small blisters on her knees that lasted for three days. She has also has noticed dysphagia for solids over the last 2 weeks. No significant muscle weakness in her extremities. ROS was otherwise negative. • PMHx: Hypothyroidism. Meds: Synthroid 0.1 mg PO QD. • PE: T:100.9, Pulse: 118, BP: 130/74, RR: 22, O2 sat: 92% with 2L O2 by nasal canula. • Chest: decreased breath sounds at the right base. • Heart: Tachycardic, no murmurs. • Joint exam: puffiness in her fingers, tenderness in her left knee. • Skin: mild mechanic hands bilaterally.
Labs • AST 41, ALT 92, Albumin 3.2, CPK 1535. • WBC: 10.5, Hb:11.9. • ANA negative, RF negative, Anti-Scl-70 negative. • Anti Jo-1 128 U (Normal < 40U). • PFTS: FVC 51% of predicted, FEV1 45% of predictive, DLCO 19% of predictive. • CTA of the chest: negative for pulmonary embolism. • High resolution Chest CT scan: Bilateral hilar lymph nodes. Lung parenchyma with bilateral opacities and ground glass opacification mainly in the lower lobes. • Lung Biopsy: No granulomatous lesions, uniform ILD with mixed inflammatory infiltrate and small areas of BOOP.
Based on her symptoms and laboratory findings patient was diagnosed with anti-synthetase syndrome.
Anti-synthetase Syndrome • The anti-synthetase syndrome is the association of inflammatory myopathy, interstitial pneumonitis, skin lesions known as “mechanic hands”, arthritis and Raynaud’s phenomenon. • Anti-synthetase antibodies are found. • These antibodies are also known as myositis-specific antibodies (MSAs). • They are directed at the cell components (proteins and ribonucleoproteins) common to every cell. • The target molecules are usually part of the protein synthetic machinery. • These antibodies are usually present at the time of the clinical presentation. • The most common of these antibodies is the anti Jo-1. • Each one of these antibodies have been associated with a particular clinical syndrome.
The Idiopathic inflammatory myopathies are a heterogeneous group of diseases. • The most common entities are Dermatomyositis, Polymyositis and Inclusion Body Myositis. • Patients with the anti-synthetase syndrome belong to a subgroup of patients with MSAs. • The most frequently found MSA is the anti Jo-1 antibody followed by anti-tRNAHis. • Anti Jo-1 antibodies are associated with the anti-synthetase syndrome. • Anti-SRP antibodies have been associated with Polymyositis with severe myalgia, arthralgia and cardiac involvement. • Anti-Mi-2 antibodies have been associated with Dermatomyositis . • The few patients with Inclusion Body Myositis and MSAs demonstrate response to immunosuppressive therapy, suggesting a better prognosis.
There are no controlled studies for this diseases. • But case reports suggest benefit with different immuno-modulators, such as azathioprine, cyclophosphamide and methotrexate. • This specific patient had a significant improvement with prednisone dosed at 1mg/kg/day and azathioprine 2 mg/kg/day.