Download
1 / 63
710 likes | 1.29k Views
SICKLE CELL TRAIT. By Cheryl Hug-English M.D., MPH October 2010. Sickle Cell Disease. Group of inherited disorders that affect red blood cells Types of Sickle Cell Disease Sickle Cell Anemia (most severe form) two sickle cell hemoglobin genes HbSS

E N D
SICKLECELL TRAIT By Cheryl Hug-English M.D., MPH October 2010
Sickle Cell Disease • Group of inherited disorders that affect red blood cells • Types of Sickle Cell Disease • Sickle Cell Anemia (most severe form) two sickle cell hemoglobin genes HbSS • HbSC (milder form) One sickle cell hemoglobin gene and one abnormal hemoglobin C gene • HbS Beta Thalassemia: One sickle cell gene and one gene for beta thalassemia (vary in severity) • HbSD, HbSO, HbSO: rare and vary in severity
Epidemiology • Sickle Cell Disease: 70,000 to 100,000 cases in the US (mostly African Americans) • Sickle Cell Disease occurs in about 1 out of every 500 African American births. • Occurs in 1 out of 36,000 Hispanic American births* *cdc.gov
Sickle Cell Disease is particularly common among people whose ancestors come from: • Sub-Saharan Africa • South America • Cuba • Central America • Saudi Arabia • India • Mediterranean countries (Turkey, Greece, Italy) • Areas of the world where malaria was a problem…sickle cell trait, less malaria http://www.cdc.gov/features/sicklecell/
100 Year History • Sickle Cell Disease first discovered and reported by Dr. James Herrick 100 years ago. • Described the experience of a young student from Grenada who came to Chicago to attend Dental School. • Developed symptoms and sought medical care. The sickled cells were first identified and reported. • “World Sickle Day June 19th 2010”: 100 years of research. http://www.cdc.gov/features/sicklecell/
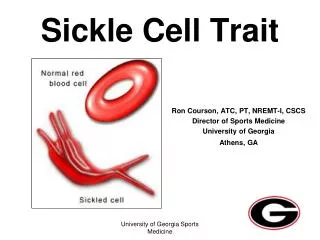
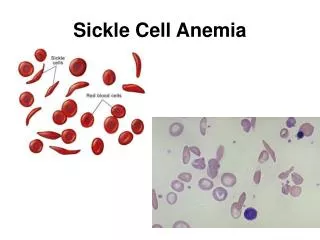
Hemoglobin • Normal hemoglobin or HbA: 4 chains; 2 alpha, 2 beta • In Sickle Cell Disease: There is a substitution of the amino acid valine for glutamic acid in the beta chain, forming what is known as HbS • Valine is more hydrophobic than glutamic acid causing the hemoglobin molecules to be attracted to one another, forming long filaments that distort the shape of the red blood cells and produce the characteristic sickling
SICKLE CELL ANEMIA • Autosomal recessive inheritance • Inherit two genes for sickle hemoglobin (HbSS) • Symptoms due to vasoocclusive symptoms from sickled cells include: • Dactylitis (acute pain and swelling in hands and feet…often the first symptom) • Fatigue, paleness, and shortness of breath • Acute Pain Crisis in any body organ or joint • Anemia • Eye problems due to decreased blood flow to retina • Jaundice • Delayed growth and puberty in children
Complications OF SCA • Infections (due to damage of spleen) • Splenic sequestration crisis • Stroke • Multi organ involvement/failure • Acute chest syndrome: chest pain, fever, abnormal CXR http://www.nhlbi.nih.gov/health/dci/Diseases/Sca/SCA_SignsAndSymptoms.html
Sickle Cell Trait • NOT Sickle Cell disease • HbAS: one gene for normal hemoglobin, one gene for hemoglobin S • Usually means about 40% of Hemoglobin in each cell is HbS • Can pass on the trait (2 people who are carriers of sickle cell trait have 25% chance of having a child with sickle cell anemia) • Most often do not have hematologic symptoms • Can lead a normal life
Epidemiology • 2million Americans carry the Sickle Cell Trait • 1 in 12 African Americans carry the Sickle Cell Trait. • Positive SCT in 8% of African Americans, 0.5% Hispanics, 0.2% Caucasians* *http://www.cdc.gov/features/sicklecell/
Why do we need to talk about SCT? • Certain circumstances or conditions can predispose individuals with SCT to have symptoms. • High altitude (flying, mountain climbing) • Increased pressure (scuba diving) • Low oxygen (when exercising intensely, training for athletic competitions, military boot camp) • Dehydation
Athletes and SCT • Identifying SCT particularly important in athletes. • High training expectations, intense workouts can make them more susceptible to having symptoms from SCT. • Despite newborn screening, many athletes do not know their Sickle Cell status. • Student Health is an ideal setting to provide screening and education for SCT
Increased Risk of Sudden Death in Sickle Cell Trait • Concern over increased risk of sudden death in PROLONGED exercise or intense training assumed to be associated with rhabdomyolysis, myocardial ischemia, and arrthymias.
Military Recruit Study • One of the first studies that looked at the risk for sudden death was done in military recruits in 1987. • Published in the New England Journal of Medicine (September 1987). • Looked at all deaths among 2 million recruits undergoing basic training from 1977 to 1981. • Unexplained death rates (per 100,000) were 32.2 in black recruits with SCT, 1.2 in black recruits without SCT, and 0.7 in white recruits without SCT. • There were 40 deaths or near deaths that were due to sickling. Most due to explosive rhadomyolysis. • Most deaths occurred after running 1-3 miles
Military Screening • US military instituted mandatory screening for sickle cell trait in 1982 • Dramatic decrease in exercise related deaths • In fact, there were no exercise related deaths in the military for the next ten years. • 1996: Military stopped mandatory screening, but individual service branches have own requirements
Sports deaths • Study done by Van Camp et al. in 1995. (Published in Med Sci. Sports Exercise May 1995) • Reviewed 160 nontraumatic deaths in high school and college athletes between 1983 and 1993. • Results showed most deaths were due to cardiovascular conditions (hypertrophic cardiomyopathy, congenital coronary artery anomalies) • BUT…7 deaths (4.4%) attributed to rhabdomyolysis and sickle cell trait.
National Athletic Trainers Report • In 2007, the NATA released a consensus statement about SCT and the Athlete • Past 4 decades sickling had been responsible for death of at least 15 football players • In past seven years sickling had been responsible for death of nine athletes: 5 college football players, two high school athletes (one a 14 year old female basketball player), two 12 year old boys training for football.
NCAA Interest in SCT • Relatively recent death…freshman defensive back Dale Lloyd at Rice in 2006 • Collapsed after running 16 sprints of 100 yards each • Cause of death was acute rhabdomyolysis • Parents sued Rice and the NCAA • This triggered the NCAA to take a closer look at this issue • 2010: NCAA issued new mandate for SCT screening
Timeline • 1974: Polie Poitier, sophomore defensive back at Univ. Colorado dies • 1975: NCAA includes section in its handbook saying “all black athletes” should be offered a sickle cell test”. • 1987: NIH recommends screening all newborns for SCD and trait. • 2001: Devaugn Darling, twin of NFL player Devard Darling dies during off season conditioning at Florida State
Timeline • 2002: Basketball player Kourtni Livingston, 14, dies in Texas after running laps • 2006: All states require screening for sickle cell trait at birth • 2007: NFL requires screening for sickle cell trait • 2007: Ryan Clark, safety for Pittsburgh Steelers has his spleen and gall bladder removed as a result of sickling after playing in a game at high elevation in Colorado • 2009: NCAA recommends testing of student athletes for sickle cell trait • 2010: NCAA mandates testing for sickle cell trait, allowing students to decline with a waiver.
What the NCAA Now Requires • Starting August 1, 2010: All Division 1 student athletes must be tested for sickle cell trait OR • Show proof of a prior test OR • Sign a waiver releasing an institution from liability if they decline to be tested • Colleges and universities are expected to provide educational information about SCT to student athletes • Divisions II and III are currently studying potential SCT testing
NCAA • This applies to incoming athletes. Returning athletes are not required to be given the test. • Transfer student athletes must receive the test. • Sickle cell testing should be done for all athletes regardless of racial or ethnicity status. • The results of the Sickle Cell test must be available before a prospective student athlete is permitted to participate.
Factors that may cause Sickling with exercise in our athletes • Severe Hypoxemia • Metabolic acidosis • Hyperthermia in muscles • Red Blood Cell dehydration
Dehydration • Dehydration causes an osmotic shift • Water leaves the RBC, causing more sickling
Hypoxemia • With intense exercise, more oxygen taken up by the muscles • Hemoglobin becomes deoxygenated • Deoxygenated hemoglobin causes sickling in RBCs more easily
Metabolic Acidosis/ Hyperthermia • Metabolic acidosis shifts oxygen dissociation curve to the right, causing hemoglobin to become deoxygenated…more sickling • Increased temperature shifts curve to the right… more sickling
What Types of Exercise have Higher risk for Sickling? • Sprinting…the harder and faster athletes run, the greater the chance for sickling (800 -1200 meters) • Many of the football deaths occurred after sprint drills or “stadium” drills
Nontraumatic Causes for Exertional Collapse • Cardiac Condition • A heat Illness • Asthma • Sickling
Sickling, Cardiac, Asthma or Heat collapse? • Cardiac Collapse: tends to be instantaneous, no cramping, inability to talk • Asthma: Slow crescendo, wheezing, chest tightness, without cramping or pain
Heat Collapse: prodrome of muscle twinges before cramping starts. Pain excruciating, muscles become locked up and rock hard. Usually occurs later in a work out with extreme heat. Body core temperature can be elevated. • Sickling Collapse: Usually occurs within first half hour onfield as during windsprints. No prodrome of muscle twinges. Muscles look and feel normal. Athlete usually collapses with muscles feeling weak. Pain not as excruciating.
Sickling vs. Heat Illness Differences • Collapse from sickling often early in a workout after sprinting activities • Heat Illness after more prolonged activity • Pain from sickling milder with weakness. Muscles feel and look normal. Athletes feel “wobbly”. • Pain from heat exhaustion excruciating with rock hard muscles..muscles lock up in full contraction. Athletes “hobble” to a stop • Sickling has no prodrome • Heat cramping often has a prodrome
Response Differences • Response differs: • 10-15 minutes after cooling, sickling pain improves. Muscles have regained oxygen and begin to function normally. • Heat cramping often takes 1-2 hours even with massage, stretching and IVs. *NATA Consensus Statement 2007
Sickling Collapse is a Medical Emergency • Fast action necessary including: • Oxygen • Cooling • Check Vital Signs • Often with these simple steps, athlete will improve • If no immediate improvement, call 911, start IV fluids, attach AED, preparing for transport • Tell hospital to be prepared for severe Rhabdomyolysis
Rhabdomyolysis • What happens with rhabdomyolyis? • Breakdown of muscle fibers • Release of protein Myoglobin into bloodstream • Myoblobin and breakdown products can cause kidney damage • Damaged muscle tissue also causes fluid to move from the blood into the muscle, leading to decreased intravascular fluid volume and decreased blood flow to the kidney
Symptoms of Rhabdomyolysis • Weakness of muscles • Fatigue • Abnormally dark urine (red or brown) • Labs: • High CPK • High serum creatinine • Positive serum myoglobin • Positive urine myoglobin • High serum potassium
Treatment • Aggressive fluid rehydration to try to prevent or minimize kidney damage • May need dialysis if severe • Correct hyperkalemia or hypocalcemia if present • Sooner treatment is begun, better prognosis
Athlete Return to Play? • Depends on severity • Athletes with mild sickling symptoms who are treated early with rest, hydration and cooling, may return to play as early as the next day. • Athletes who have had true rhabdomyolysis with hospitalization and dialysis may never return to play due to kidney damage • In between: those who have elevated creatinekinase, but no elevation in serum creatinine or indication of kidney damage, may have muscle weakness and soreness for a week or two. May return to play gradually.
Precautions for Athletes with SCT • Build up slowly in training with paced progressions • Allow longer periods of rest and recovery between repetitions • Encourage participation in preseason strength and conditioning programs • Athletes with SCT should be excluded from participation in performance tests such as mile runs, serial sprints etc.
Precautions • Stop activity with onset of symptoms (cramping, pain, weakness, inability to catch breath, fatigue) • All athletes with SCT to set their own pace • Adjust work cycles for environmental heat stress, emphasize hydration, no workout if an athlete with SCT is ill, modify training when at high altitude • Encourage athlete to report any symptoms immediately
Testing methods • Screening: • Hemoglobin S solubility test: (Sickledex) Older test. Add chemicals to patient’s blood sample that reduces amount of oxygen. Can detect HbS, but does not distinguish between SCD and SCT. Should not be used in infants less than 6 months (still have HbF). • If this test is used, any positives should be evaluated further with Hb electrophoresis.
Hemoglobin Evaluation: • To identify types and relative amounts of various hemoglobins • These tests separate the hemoglobins so that they can be quantified. • Hemoglobin Electrophoresis • Hemoglobin Fractionation by HPLC (high pressure liquid chromatography) • Isoelectric focusing
Screening Program at UNR • Although NCAA mandated SCT screening in 2010, at the University of Nevada, Reno we started looking at this issue in 2008. • In 2008, we had done SCT testing on athletes with problems with cramping. Identified 10 athletes who had SCT. • In 2009, initiated voluntary screening for SCT for all athletes. • Summer 2010, mandatory screening of all athletes
Initial Steps for UNR Screening Program • Steps: • Informed consent obtained from student athlete prior to the blood draw. • Option 1: undergo blood test • Option 2: provide documentation and results of previous testing • Option 3: Written refusal of test
Steps • All SCT results given to Head Team Physician. • Results (both positive and negative) are recorded on the pre-participation exam form. • All student athletes with a positive SCT result are scheduled to have a follow up visit with head team physician. • Informational handouts on SCT given to student athlete as part of visit. • Counseling and/or Genetic counseling is also provided as needed. • Positive results communicated to the Athletic Trainer, Head and Assistant coaches, and strength and conditioning coaches for the particular sport the student athlete is involved in.
Recommended Changes in routineShared with Coaches, Trainers • Stress the importance of immediately reporting symptoms (e.g. difficulty breathing, fatigue, muscle cramping or pain in lower back or leg, sudden weakness, swelling, tenderness) to athletic trainers, coaches, and staff. • Stop activity with onset of any symptoms. • Gradual build up in lifting and conditioning training with extended periods of rest and recovery, especially between repetitions. • Exclude from participation in “preseason conditioning tests”.
Modification of conditioning drills (no timed sprints, no sustained running without periods of rest). • Discontinue all-out exertion activities of any kind lasting beyond 2 to 3 minutes without breathers. • Allow student-athlete to set his/her own pace. • Emphasize hydration and implement a hydration policy for before, during, and after all activities. • Emphasize control of any asthma, which can worsen the sickling effect.
Adjust work/rest cycles for heat stress and altitude acclimatization. Modify activity in extremely hot and humid conditions. • Allow no workout if student-athlete is ill, especially illnesses involving fever, diarrhea or vomiting. • Encourage pre-conditioning prior to returning to the sport each season. • Modify activities after nights of poor sleep.
Participation • The student athlete will be allowed to participate after appropriate counseling • Recommendation will be provided as to clearance for participation in intercollegiate athletics or follow-up as deemed necessary.