Download
1 / 56
760 likes | 2.59k Views
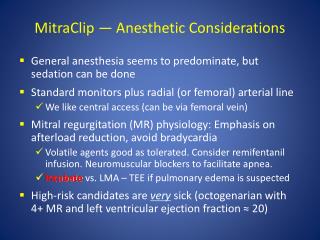
INTRODUCTION TO ANESTHESIA & PRE-ANESTHETIC AGENTS. CHAPTERS 1 & 3. TERMINOLOGY OF ANESTHESIA. Anesthesia may be defined as “loss of sensation”, but this only describes one of its effects.

E N D
INTRODUCTION TO ANESTHESIA & PRE-ANESTHETIC AGENTS CHAPTERS 1 & 3
TERMINOLOGY OF ANESTHESIA • Anesthesia may be defined as “loss of sensation”, but this only describes one of its effects. • It is used daily in most veterinary practices to provide sedation, tranquilization, immobility, muscle relaxation, unconsciousness, and pain control for a diverse range of indications including surgery, dentistry, grooming, diagnostic imaging, wound care, and capture/transport of wild animals
TERMINOLOGY OF ANESTHESIA • Sedation refers to drug-induced CNS depression and drowsiness that vary in intensity from light to deep. • Patient can be aroused by noxious stimuli • Tranquilizaionis a drug-induced state of calm in which the patient is reluctant to move and is aware of but unconcerned about its surroundings. • Often used interchangeable with sedation
TERMINOLOGY OF ANESTHESIA • Hypnosis is a sleeplike state from which the patient can be aroused with sufficient stimulation. • Narcosis refers to a drug-induced sleep from which the patient is not easily aroused and that is most often associated with the administration of narcotics.
TERMINOLOGY OF ANESTHESIA • General anesthesia may be defined as a reversible state of unconsciousness, immobility, muscle relaxation, and loss of sensation throughout the entire body produced by administration of one or more anesthetic agents. • Surgical anesthesia is a specific stage of general anesthesia in which there is sufficient degree of analgesia(loss of sensitivity to pain) and muscle relaxation to allow surgery to be performed without patient pain or movement.
Fully conscious Awake Light sedation Moderate sedation Sedation Deep sedation Border between Consciousness and unconsciousness Hypnosis Narcosis Light surgical anesthesia Unconscious Moderate surgical anesthesia General anesthesia Deep surgical anesthesia Anesthetic overdose
TERMINOLOGY OF ANESTHESIA • Local anesthesia refers to loss of sensation in a small area of the body produced by administration of a local anesthetic agent in proximity to the area of interest. • Topical anesthesia is the loss of sensation of a localized area produced by administration of a local anesthetic directly to a body surface or to a wound. • Regional anesthesia refers to a loss of sensation in a limited area (larger area than with local anesthetics)of the body produced by administration of local anesthetic agent in proximity to sensory nerves.
TERMINOLOGY OF ANESTHESIA • Balanced anesthesia refers to the practice of administering multiple drugs concurrently in smaller quantities than would be required if each were given alone. • Maximizes benefits of each drug • Minimizes adverse effects • Allows anesthetist to produce CNS depression, immobilization, and pain relief that is appropriate for the patient and the procedure.
PRE-ANESTHETIC AGENTS & ADJUNCTS • ANESTHETIC AGENT: any drug used to induce a loss of sensation with or without unconsciousness. • ADJUNCTS: a drug that is not a true anesthetic but that is used during anesthesia to produce other desired effects such as sedation, muscle relaxation, analgesia, reversal, neuromuscular blockade, or parasympathetic blockade • Ex: muscle relaxants, neuromuscular blockers, reversal agents
PRE-ANESTHETIC AGENTS & ADJUNCTS • CHOOSING THE APPROPRIATE AGENTS • AVAILABILITY: most clinics will not have the option of choosing from every drug on the market. • FAMILIARITY: drugs are often chosen based on the veterinarian’s familiarity • PROCEDURE: drugs that are appropriate for one procedure may not be appropriate for another • Some drugs are short-acting and would not be appropriate for long surgeries • Some drugs may be appropriate for a spay but not a c-section
PRE-ANESTHETIC AGENTS • COST: It is ok to use a cheaper anesthetic as long as it is just as safe as the more expensive one. • TIME TO ONSET OF ACTION: in emergency situations, fast-acting drugs may be necessary • The anesthetic protocol, dose, and route are chosen by the veterinarian • Many clinics have a routine protocol, but is important to consider all aspects of the patient’s minimum database
PRE-ANESTHETIC AGENTS • Drugs that are administered to an animal prior to general anesthesia • May be a single drug or combination of drugs • Do not mix two or more drugs unless you have reliable evidence that it is safe to do so. • REASONS TO ADMINISTER PRE-ANESTHETIC AGENTS • To calm or sedate an excited or fractious animal
PRE-ANESTHETIC AGENTS • REASONS TO ADMINISTER PRE-ANESTHETIC AGENTS • To counteract the effects of other injectable or inhalant anesthetics • Ex: some anesthetic agents cause hypersalivation, we can use atropine or glycopyrrolate to counteract this effect. • To reduce the amount of general anesthetic agents required • If the patient is already sedated, it takes less drug to bring them into the unconscious state. This is a safer practice than using large amounts of drugs • Using smaller amount of both pre-anesthetics and anesthetic agents in combination is known as balanced anesthesia.
PRE-ANESTHETIC AGENTS • REASONS TO GIVE PRE-ANESTHETIC AGENTS • To reduce pain & discomfort: some pre-anesthetic agents last long enough to be effective post-operatively
CLASSES OF PREANESTHETIC AGENTS • ANTICHOLINERGICS • TRANQUILIZERS and SEDATIVES • Phenothiazines • Benzodiazepines • Alpha-2 agonists • OPIODS • Agonists • Partial agonists • Agonist-antagonists • antagonists
ANTICHOLINERGICS aka parasympatholytics or sympathomimetics
ANESTHETIC & SURGICAL TECHNIQUES MAY STIMULATE THE VAGUS NERVE • The vagus nerve provides parasympathetic innervation to numerous target organ such as: • Heart • Lungs • GI tract (viscerovagal reflex) • Secretory glands • Iris(oculovagal reflex) • When the vagus nerve is stimulated by endotracheal intubation, GI traction, or manipulation of the eye, what effect does it have on the organs above?
ANTICHOLINERGICS • Acetylcholine is the primary neurotransmitter in the PNS responsible for parasympathetic effects (cholinergic effects) Ach Ach
ANTICHOLINERGICS These drugs are given to counteract the effects caused by vagal stimulation EXAMPLES: Atropine, Glycopyrrolate
ANTICHOLINERGICS Ach Ach ANTICHOLINERGICS ONLY AFFECT MUSCARINIC RECEPTORS ON THE TARGET ORGANS
WHAT EFFECT DO ANTICHOLINERGICS HAVE ON THE VARIOUS BODY SYSTEMS? EFFECTS: ADVERSE EFFECTS:
WHAT EFFECT DO ANTICHOLINERGICS HAVE ON THE VARIOUS BODY SYSTEMS? EFFECTS: ADVERSE EFFECTS:
WHAT EFFECT DO ANTICHOLINERGICS HAVE ON THE VARIOUS BODY SYSTEMS? EFFECTS: ADVERSE EFFECTS:
WHAT EFFECT DO ANTICHOLINERGICS HAVE ON THE VARIOUS BODY SYSTEMS? EFFECTS: ADVERSE EFFECTS:
WHAT EFFECT DO ANTICHOLINERGICS HAVE ON THE VARIOUS BODY SYSTEMS?
WHAT EFFECT DO ANTICHOLINERGICS HAVE ON THE VARIOUS BODY SYSTEMS?
WHAT EFFECT DO ANTICHOLINERGICS HAVE ON THE VARIOUS BODY SYSTEMS?
ATROPINE vs. GLYCOPYRROLATE: A COMPARISON • Both drugs can be given SQ or IM (preanesthetic purposes) or IV (emergency treatment of bradycardia/cardiac arrest) • Atropine is generally preferred for emergencies due to the quicker onset of action • Onset of Action/Duration of Action • Atropine IM: 5min, peak @ 10-20min, duration 60-90min • Atropine IV: 1 min, peak @ 3-4 min, duration several minutes • Glycopyrrolate IM: similar onset time to atropine, peak @ 30-45min, duration 2-3 hrs
ATROPINE vs GLYCOPYRROLATE: A COMPARISON • Glycopyrrolate causes less tachycardia • Glycopyrrolate is better at decreasing salivation • TOXICITY • With overdoses drowsiness, excitement, dry mouth, ataxia, muscle tremors, dilated pupils, hyperthermia, and tachycardia may be seen • REVERSED with PHYSOSTIGMINE • Reversal is uncommon • ANTICHOLINERGICS ARE NOT CONTROLLED
TRANQUILIZERS and SEDATIVES PHENOTHIAZINES BENZODIAZEPINES ALPHA-2 AGONISTS
GENERAL INFO ON TRANQUILIZERS/SEDATIVES • Tranquilizers reduce anxiety, but may not decrease awareness • Sedatives reduce mental activity and awareness and induce sleepiness These terms are often used interchangeably • Patients that have received a tranquilizer/sedative may still be easily aroused and could potentially get aggressive or injure themselves http://www.youtube.com/watch?v=AkaGWwTHD5g
PHENOTHIAZINES ACEPROMAZINE CHLORPROMAZINE
GENERAL INFO on PHENOTHIAZINES • These drugs have no analgesic effects • These drugs are not controlled • These drugs do not have a reversal agent • Examples: Acepromazine, Chlorpromazine
WHAT ARE THE EFFECTS THAT PHENOTHIAZINES HAVE ON THE VARIOUS BODY SYSTEMS? EFFECTS: ADVERSE EFFECTS: EFFECTS: ADVERSE EFFECTS:
WHAT ARE THE EFFECTS THAT PHENOTHIAZINES HAVE ON THE VARIOUS BODY SYSTEMS? EFFECTS: ADVERSE EFFECTS: EFFECTS: ADVERSE EFFECTS:
OTHER EFFECTS & ADVERSE EFFECTS of PHENOTHIAZINES: • ANTIHISTAMINE EFFECT • PENILE PROLAPSE • DECREASED PCV • Onset of action/duration of action • 15min after IM injection, peak@ 30-60 min • Duration: 4-8 hrs( could be up to 48hrs)
THINGS TO CONSIDER WITH PHENOTHIAZINES • Sedative effects can be overridden if patient is stimulated to a sufficient degree • Use a max of 3mg in dogs and 1mg in cats • Boxers and giant breed dogs by have increased sensitivity • Terriers and cats are more resistant to its effects • Chlorpromazine is used in veterinary medicine as an antiemetic, but not as an anesthetic adjunct.
BENZODIAZEPINES DIAZEPAM MIDAZOLAM ZOLAZEPAM
GENERAL INFO ON BENZODIAZEPINES • Benzodiazepines depress the CNS by increasing activity of endogenous gamma-aminobutyric acid (GABA), an inhibitory neurotransmitter in the brain. • These drugs are controlled • These drugs can be reversed • Flumazenil is the benzodiazepine antagonist. It is rarely used due to the very low incidence of adverse effects and the high cost. • These drugs provide no analgesia • These drugs have unreliable sedative effects & could induce dysphoria, excitement, or ataxia in young, healthy animals, esp. when given alone • EXAMPLES: DIAZEPAM, MIDAZOLAM, ZOLAZEPAM
WHATEFFECTS DO BENZODIAZEPINES HAVE ON THE VARIOUS SYSTEMS OF THE BODY? EFFECTS: EFFECTS: ADVERSE EFFECTS:
WHAT EFFECTS DO BENZODIAZEPINES HAVE ON THE VARIOUS SYSTEMS OF THE BODY? EFFECTS: EFFECTS:
THINGS TO CONSIDER ABOUT BENZODIAZEPINES • Diazepam is not water-soluble and cannot be mixed with water-soluble agents except ketamine • Midazolam and zolazepam are water-soluble and can be mixed with other agents • Diazepam is is painful and poorly absorbed when administered intramuscularly • Midazolamis more readily absorbed via IM and SQ routes • Zolazepam is available only mixed with tiletamine to produce the combination product Telazol. • Diazepam is very soluble in plastic and over time is absorbed by syringes, IV bags, and IV tubing
THINGS TO CONSIDER ABOUT BENZODIAZEPINES • Diazepam and midazolam are light-sensitive • Onset of action/duration of action • Less than or equal to 15 min after IM injection • Duration: 1-4 hours
ALPHA-2 AGONISTS XYLAZINE DEXMEDETOMIDINE
GENERAL INFO ON ALPHA-2 AGONISTS • These drugs are not controlled • These drugs can be reversed • These drugs do provide analgesic effects • These drugs act on alpha-2 adrenergic receptors in the CNS and PNS causing a decrease in the neurotransmitter norepinephrine
WHAT EFFECTS DO ALPHA-2 AGONISTS HAVE ON THE VARIOUS BODY SYSTEMS? EFFECTS: ADVERSE EFFECTS: EFFECTS: ADVERSE EFFECTS:
WHAT EFFECTS DO ALPHA-2 AGONISTS HAVE ON THE VARIOUS BODY SYSTEMS? EFFECTS: ADVERSE EFFECTS: EFFECTS: ADVERSE EFFECTS:
OTHER EFFECTS OF ALPHA-2 AGONISTS • Hyperglycemia: alpha-2 agonists reduce the secretion of insulin by the pancreas • Hypothermia: alpha-2 agonists decrease thermoregulation and shivering • Premature parturition • Can be absorbed through the skin and abrasions – as little as 0.1ml of dexmedetomidine can cause hypotension and sedation in humans.
THINGS TO CONSIDER ABOUT ALPHA-2 AGONISTS • Xylazine is largely reserved for use in large animals • Cattle are sensitive and only require 1/10 of the dose used in horses • Dexmedetomidine is largely used in small animals and is more potent than xylazine • Both drugs are commonly mixed with other drugs such as ketamine, and an opioidsuch as butorphanol or morphine • Animals can undergo minor and major surgical procedures with these combinations
THINGS TO CONSIDER ABOUT ALPHA-2 AGONISTS • These drugs can be reversed with Yohimbine (reverses xylazine) and Atipamezole (reverses dexmedetomidine) • Atipamezole is sold in combination with dexmedetomidine and is given in a 1:1 ratio • It is not recommended to treat bradycardia with anticholinergics, but rather the appropriate reversal agent • Reversal takes only 5-10min