Download
1 / 64
670 likes | 1.05k Views
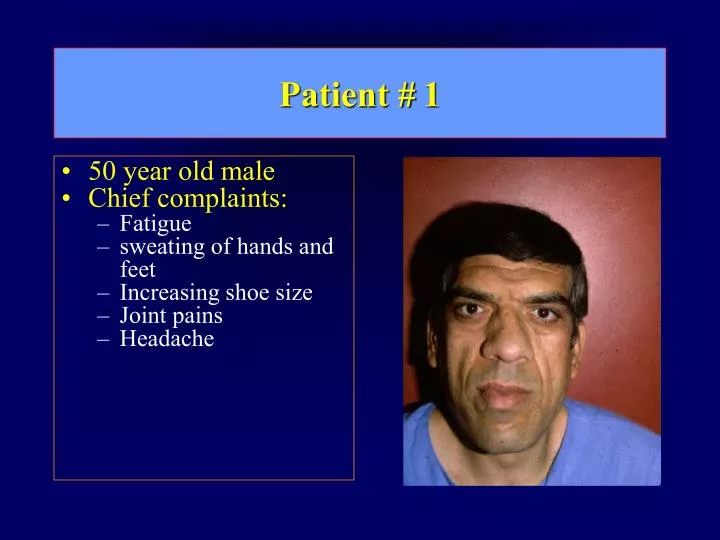
Patient # 1. 50 year old male Chief complaints: Fatigue sweating of hands and feet Increasing shoe size Joint pains Headache. Patient #1 (2). Pertinent family history No family history of Pituitary tumors Hypercalcemia Pancreatic tumors Past medical history

E N D
Patient # 1 • 50 year old male • Chief complaints: • Fatigue • sweating of hands and feet • Increasing shoe size • Joint pains • Headache
Patient #1 (2) • Pertinent family history • No family history of • Pituitary tumors • Hypercalcemia • Pancreatic tumors • Past medical history • s/p carpal tunnel surgery • Physical findings
GH Excess Enlargement of hands and feet Thick skin Skin tags Sweating Sleep Apnea Carpal Tunnel Syndrome Glucose intolerance Osteoarthritis Colonic Polyps Tumor-related Headache Visual field defect Loss of pituitary function Gonadotrophins TRH - hypothyroid ACTH - Addison’s Acromegaly - Signs and Symptoms
Acromegaly Frontal Bossing Chin Protrusion
Acromegaly A patient with marked macroglossia. This can cause severe sleep apnea which can be associated with cardiac arrhythmias and sudden death.
Dopamine Glucose Alpha adrenergic Opiates GABA + Regulation of GH Secretion TRH SS GRH GH Stimulation IGF-1 Inhibition
Post Prandial Acromeg. Control Screening Growth Hormone Levels in Acromegaly Fasting GH Upper “Normal” Acromeg. Control
Additional Tests to Diagnose Acromegaly • IGF-1 (Insulin-like Growth Factor 1) • IGF-BP3 (IGF binding protein 3) • Advantages: • Single blood level • No diurnal variation • Disadvantages • Some overlap with normal
Definitive Test for Acromegaly • Oral Glucose Tolerance Test (OGTT)
Acromegaly Control Oral Glucose Tolerance Test GH Upper “Normal” 0 30 60 90 1200 Time (minutes)
Acromegaly: Diagnosis Clinical suspicion of acromegaly 1-2hr postprandial GH, IGF1 and IGFBP3 Normal Abnormal 2 hr OGTT with GH levels Normal Acromegaly Excluded Abnormal Acromegaly diagnosed
Growth-Hormone ExcessEtiology • 98%: GH-producing pituitary tumor • 2%: Ectopic GHRH secretion • Small cell lung cancer • Bronchial or intestinal carcinoid tumors • Pancreatic islet cell tumor • Pheochromocytoma
Acromegaly: Diagnosis Clinical suspicion of acromegaly 1-2hr postprandial GH, IGF1 and IGFBP3 Normal Abnormal 2 hr OGTT with GH levels Normal Acromegaly Excluded Abnormal Pituitary MRI Normal Octreoscan Abnormal Site-specific CT/MRI TREATMENT
Pituitary Macroadenoma (Sagittal MRI Scan) Optic Chiasm Pituitary Tumor
Normal Visual Fields 90 70 50 50 70 90 O.S. O.D.
Bitemporal hemianopsia due to Pituitary Tumor 90 70 50 30 30 50 70 90 O.S. O.D.
Visual Field Defects Caused by Pituitary Tumor From Sandoz slide set
Acromegaly (1) • Prevalence: 40-50 / 106 • Incidence: 3-4 / 106 • Mean age of onset: 32 years • Mean age at diagnosis: 42 years • Prognosis: 2x increased mortality if not treated • Cure rate: Greatly reduced if tumor invades cavernous sinus
Acromegaly: Treatment options Transsphenoidal Surg. Radiotherapy Somatostatin Dopaminergic Micro Macro Analog (Cabergoline) GH <1 mcg/l Normal IGF1 82% 47% 75% (20 years) 50-65% 10-20% Recurrence 5-10% * Late response inconv. & cost Low efficacy Complications Hypopit. 15% >50% None None Other DI- 2-3% Neuro deficits Gallstones Nausea, hypotens. * At 10 years, Longer-term recurrence probably higher
Dopamine Glucose Alpha adrenergic Opiates GABA + Regulation of GH Secretion TRH SS GRH GH Stimulation IGF-1 Inhibition
Pegvisomant - GH receptor antagonist Normalization of GH 90% Normalization of IGF1 80-90% Tumor growth Rare Long-term effect Unknown
Invasive Acromegaly: Treatment Algorithm Pituitary Adenoma < 1 cm >1 cm Consider preoperative somatostatin analog Transphenoidal surgery Post prand GH >1 mcg/l And/or IGF-1 elevated Post-prand. GH <1 mcg/l IGF-1 normal somatostatin analog or dopaminergic Progressive therapy if post-prand. GH >1 mcg/l and IGF-1 not normal somatostatin analog, GHR antagonist or dopaminergic Annual Follow-up Combination therapy Adapted from Melmed ESAP, 1999 Radiation Therapy
Patient #3 • 35 year old woman • Chief complaint • Amenorrhea for 6 months • Galactorrhea • Otherwise healthy • Past medical history • Family History • Physical findings
Patient #3 • Prolactin -- 5000 pmol/l (nl < 900 pmol/l) • CT - consistent with microadenoma
Differential Diagnosis of Hyperprolactinemia • Medications • Alpha-methyldopa, reserpine • Phenothiazines, butyrophenones, • benzamides (metoclopramide, sulpride) Estrogens • H2-receptor blockers (cimetidine) • Opiates • Hypothyroidism • Decreased dopamine delivery to pituitary • Pituitary, suprasellar and hypothalamic lesions • Radiation damage to the hypothalamus
Differential Diagnosis of Hyperprolactinemia • Prolactin levels > 11,000 pmol/l is usually indicative of macroprolactinoma. • Stalk compression, medications, hypothyroidism and stress usually result in prolactin levels < 2,000 and virtually always less than 6,500 pmol/l. • Microprolactinomas, mass lesions compressing the pituitary stalk frequently present with similar prolactin levels.
Women: Amenorhea 57-90 % Oligomenorrhea 10-28 % Regular menses 9-15 % Galactorrhea 30-80 % Headache 40 % Visual field defect<25 % Hirsutism 19 % Men: Decreased libido 75-100 % Impotence 68-100 % Headache 70 % Visual field defect 36-70 % Galactorrhea 10-30 % Gynecomastia 4-50 % Hyperprolactinemia: Clinical Presentation
Response Recurrence Surgery Microprolactinoma 60-80% 50% Macroprolactinoma 10-30% ~100% RadiotherapyNormalization of PRL after ~10 years Medical Therapy Microprolactinoma >90% Macroprolactinoma 50-80% Prolactinoma: Results of Treatment
Clinical Evaluation of Hyperprolactinemia Increased fasting, resting prolactin levels < 6,500 pmol/l > 6,500 pmol/l Exclude: Stress Renal failure Medications Hypothyroidism CT or MRI CT or MRI "Non-functioning" macroadenoma Micro- prolactinoma Macro- prolactinoma Surgery and/or Radiation Dopaminergic Therapy
Patient #3: A.L. - History • 58 year old male • Presenting symptoms (3 months): • Decreased vision • Weight loss • Nausea • Dizziness • Impotence • Occasional diarrhea • Physical examination: • Bitemporal hemianopsia • Atrophic testes
A.L. - Laboratory Data • Blood count, electrolytes, liver and kidney functions - Normal • Endocrine tests: • Prolactin - 50,400 pmol/l (N <450) • T4 - 46 nmol/l (N 60 - 160) • T3 - 2.0 nmol/l (N 1.2 - 3) • TRH test: TSH increased from 1.2 to 7.2 mU/l with delayed curve • ACTH test: Cortisol 108 to 617 µmol/l @ 60 minutes (Normal basal 200-700) • Testosterone - <0.9 nM/l (Nl 7-30) • LH - 4.1 U/l (3-15) • FSH - 1.2 U/l (1-10)
Optic Chiasm Pituitary Macroadenoma AL- Pre-treatment MRI
A.L. - Pre-treatment Visual Fields 24/3/89 O.S. O.D.
A.L. - Treatment • Diagnosis: • Macroprolactinoma • Hypopituitarism: • Thyroid axis • Adrenal axis • Gonadotrophin axis • Treatment: • Postpone surgery • Bromocriptine in increasing doses • Cortisol, thyroid and testosterone replacement
80,000 30 Prolactin (pmol/l) 25 Bromocriptine (mg/d) 60,000 20 Prolactin pmol/l Bromocriptine Dose (mg/d) 40,000 15 10 20,000 5 0 0 April-90 Aug-89 April-89 Jan - 93 Dec-91 A.L. - Prolactin Levels During Treatment
A.L. - Post-treatment Visual Fields 26/10/89 O.S. O.D.
Optic chiasm AL- MRI Post-treatment
A.L. - Long-term Follow-up • CT, MRI: • Complete tumor regression - empty sella • Complete normalization of visual fields • Pituitary functions: • Complete normalization of all axes • Prolactin levels: • 130 - 650 pmol/l (N < 450) on 1.25 - 0.625 mg/d bromocriptine
Pt# 4 • 55 year old male • Coma • Blood pressure normal, no edema • Hyponatremia • Normokalemia • Past medial history • Viral syndrome 2 days before entry • Weight loss • Nausea • Progressive impotence, weakness and fatigue • Not taking any medications • Liver/Kidney function normal • Chest x-ray normal
Patient #4 (2) • Additional tests: • Urine sodium -- 50 mEq/l • Presumptive Diagnosis
Syndrome of Inappropriate ADH (SIADH) • Clinical findings: • Hyponatremia • Euvolemia (mild volume expansion) • Normokalemia • Diagnosis: • Hyponatremia • Inappropriately elevated urine sodium • No volume depletion or severe volume expansion • Etiology: • Glucocorticoid deficiency • Hypothyroidism • Pulmonary lesions • CNS lesions • Drugs (Chlorpropamide and others)