Download
1 / 23
240 likes | 280 Views
Learn about posterior surgery for cervical spondylotic myelopathy, including indications, comparison with anterior surgery, importance of compression site and curve, patient factors, complications, advantages, and specific case studies. Make informed decisions about anterior vs. posterior surgery for the best outcomes.

E N D
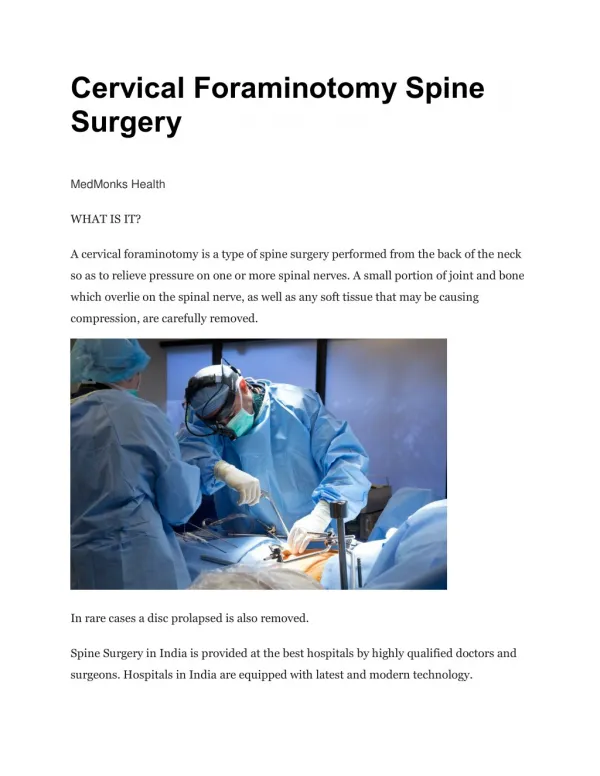
Posterior surgery for Cervical Spondylotic MyelopathyMehmet Zileli, M.D. Izmir - Turkey
CSM Posterior Decompression • Indications • Posterior compression • >2 level anterior compression • Hyperlordosis • Contraindications • Kyphosis • 1-2 level anterior compression
Anterior vs Posterior Surgery?Decision Making 1-Site of compression 2-Cervical curve 3-Number of compressions 4-Patient’s general condition, bone quality
Anterior vs Posterior Surgery?Importance of Site of Compression Anterior compression • Anterior surgery Posterior compression • Posterior surgery Anterior & posterior compression • ??? • The number of levels ? • Instability ?
Anterior vs Posterior Surgery?Importance of Curve • Kyphotic curve • Anterior surgery • Multiple levels ?? • Hyperlordotic curve • Posterior surgery • Lordosis preserved - lost • ???
Anterior vs Posterior Surgery?Patient’s age, general condition, bone quality • Age is not a factor alone • Graft problems if osteoporotic • Poor general condition • Posterior surgery > Anterior surgery
Complications of Anterior Surgeryappr. 20-25% 1-Neurological complications 2-Cervical site compl. Airway problems Hematom Esophageal injury Vascular Hoarseness Dysphagia Chylothorax 3-Graft related compl. Graft dislocation Pseudarthrosis Adjacent level degeneration Plate & screw problems 4-Graft site compl.
CSM: Posterior Surgery Advantages 1-Very good technique for decompression of structures from posterior such as ligamentum flavum hypertrophy. Disadvantages 1-Increasing instability resulting in osteophyte formation 2-Hard discs and anterior osteophytes are not possible to remove, if attempted, it would cause root injury 3-Neurological complications are more in comparison to anterior surgery
Posterior SurgeryAbsolute Indications 44 y.o. male, quadriparesis for 5-6 yrs, gait disturbance for 1 yr, sphincter disturbancePosterior compression only > posterior surgery
Posterior SurgeryAbsolute Indications 79 y.o. Female, walking disturbance for years. Inability to walk for 1 month, wheel-chair dependent. MRI: severe anterior and posteriorcompression at C3-4. Coronary artery disease, high risk for cardiac reasons
Posterior SurgeryRelative Indications 72 y.o. Male. Tetraparesisi prominent on right side for 1 year. MRI C4-5-6-7 severe narrowing T2 hyperintensity , lordoticcurve.
3 levels anterior-posterior compression, lordosis is preserved > posterior surgery Postop MRI
CSM: Posterior Surgery Laminectomy & Fusion Lateral mass fixation Laminoplasty Hemilateral opening Bilateral opening
Laminectomy & Fusion Lateral mass fixation
Laminoplasty • Unilateral opening • Bilateral opening
Laminectomy or Laminoplasty? Laminectomy Causes instability Laminectomy membrane Laminoplasty Technically demanding Restricted neck movements Insufficient decompression?
OutcomeAnterior vs Posterior • Success rates range between 70-85% in different series • Duration of symptoms are important
ComplicationsAnterior vs Posterior • Functional outcomes similar • But complications greater with corpectomy Yonenobu, et. al. – Spine, 1992 Heller, et. al. – Spine, 2001 Wada, et. al. – Spine, 2001 Edwards, et.al. – Spine, 2002
Conclusions For multi-level anteriorcompression < 2 Levels Multi-level ACDF 2 Levels Corpectomy >2 Levels Laminectomy or Laminoplasty For multi-level diffuse (e.g. congenital) compression • No Kyphosis Laminoplasty or corpectomy • Kyphosis Corpectomy
Conclusions • With proper indications, results comparable with either corpectomy or laminectomy / laminaplasty • Higher complication rate with corpectomy
CSM Posterior Decompression • Indications • Posterior compression • >2 level anterior compression • Hyperlordosis • Contraindications • Kyphosis • 1-2 level anterior compression