Download
1 / 44
450 likes | 843 Views
Mental Capacity Act Update 2010. Dr Jonathan Waite FRCPsych LLM Nottinghamshire Healthcare NHS Trust QMC Campus Jonathan.Waite@nottshc.nhs.uk. Mental Capacity Act 2005 2005 Chapter 9. Mental Capacity Act 2005.

E N D
Mental Capacity ActUpdate 2010 Dr Jonathan Waite FRCPsych LLM Nottinghamshire Healthcare NHS Trust QMC Campus Jonathan.Waite@nottshc.nhs.uk
Mental Capacity Act 2005 2005 Chapter 9 Mental Capacity Act 2005 An Act to make new provision relating to persons who lack capacity; to establish a superior court of record called the Court of Protection in place of the office of the Supreme Court called by that name; to make provision in connection with the Convention on the International Protection of Adults signed at the Hague on 13th January 2000; and for connected purposes.
Mental Health Act 2007 2007 Chapter 12 Mental Health Act An Act to amend the Mental Health Act 1983, the Domestic Violence, Crime and Victims Act 2004 and the Mental Capacity Act 2005 in relation to mentally disordered persons; and for connected purposes.
Ilkeston ADVERTISER Published on Mon Jul 12 19:32:26 BST 2010 • Health chiefs have vowed to learn lessons from the death of a Trowell woman who died after forgetting to take vital medication. • Investigations were launched by the Derbyshire PCT and Nottinghamshire County Council after 85-year-old Olive Martin died and bosses say steps have since been taken to ensure the same thing does not happen again. • Coroner for Nottingham, Dr Nigel Chapman, held an inquest into her death and said that he wanted to 'force agencies to look at what they do' after the tragedy.
Ilkeston ADVERTISER Published on Mon Jul 12 19:32:26 BST 2010 • Mrs Martin was given the medication by her GP practice at Ilkeston Health Centre but her case was transferred to Littlewick Medical Centre, in Ilkeston, in June 2009. They started issuing prescriptions without any knowledge of Mrs Martin's medical history. Haley Disney, a district nurse from the practice visited Mrs Martin's home in August and noticed a dose had been missed.
Ilkeston ADVERTISER Published on Mon Jul 12 19:32:26 BST 2010 • She reported this to Littlewick Medical Centre and ordered an extra dose from the pharmacy and left a note for Mrs Martin's evening carer to prompt her to take the Warfarin. But the carer told the inquest she was not allowed to prompt Mrs Martin to take Warfarin, due to the strength of the drug. She advised Mrs Martin to call Littlewick Medical Centre and left a note to the district nurse and the care agency Claimar. But the inquest heard no-one from Littlewick returned Mrs Martin's calls.
Ilkeston ADVERTISER Published on Mon Jul 12 19:32:26 BST 2010 • On September 13, Mrs Martin was taken to the City Hospital with chest pains and died later that night. Dr Chapman recorded a verdict of natural causes.
Tort • Assault - An act committed intentionally or recklessly which leads another person to fear immediate personal violence • Battery - The direct or indirect application of unlawful force by one person on another • Negligence - The breach by the defendant of a legal duty of care which results in damage to the plaintiff
Duty of care (GMC) The three main duties of care of a doctor are: To protect life and health, To respect autonomy and To treat justly. These duties can conflict. For example, the duty to respect autonomy means that a competent adult has the right to refuse treatment, even if to do so will result in death. The duty to protect life and health is not absolute; the availability of modern technology to maintain life does not mean that it should always be applied if, for example the overall consequence might be to cause distress in a patient who was dying
Consent (GMC) • You must be satisfied that you have consent or other valid authority before you undertake any examination or investigation, provide treatment or involve patients in teaching or research. • Usually this will involve providing information to patients in a way they can understand, before asking for their consent. • You must follow the guidance in “Seeking Patients’ Consent: The ethical considerations,”which includes advice on children and patients who are not able to give consent.
Code of Practice • The Code of Practice (Code) provides guidance on how the Mental Capacity Act 2005 (Act) works on a day-to-day basis. • It has case studies and explains in more detail what the key features of the law are. • Certain categories of people have a legal duty to have regard to the Code. This includes:
Code of Practice • Professionals and anyone who is paid for the work they do in relation to people who lack capacity e.g. Doctors, nurses, social workers, care managers, solicitors, police officers, ambulance crew and paid carers; • Attorneys appointed under a Lasting Power of Attorney (LPA) or Enduring Power of Attorney (EPA); and • Deputies appointed by the Court of Protection (Court). Family, friends and unpaid carers do not have a duty to ‘have regard’ to the Code but will still find the guidance helpful.
Mental Capacity Act 2005 • s.1 Principles • s.2 People who lack capacity • s.3 Unable to make a decision • s.4 Best Interests • s.5 Acts in connection with care or treatment • (General Authority to act reasonably) • s.6 s.5 Acts: Limitations • s.7 Payment for necessary goods and services • s.8 Expenditure
1. The Principles (1)The following principles apply for the purposes of this Act. (2) A person must be assumed to have capacity unless it is established that he lacks capacity. (3) A person is not be treated as unable to make a decision unless all practicable steps to help him to do so have been taken without success. (4) A person is not be treated as unable to make a decision merely because he makes an unwise decision. (5) An act done, or a decision made, under this Act for or on behalf of a person who lacks capacity must be done, or made, in his best interests. (6) Before the act is done, or the decision is made, regard must be had to whether the purpose for which it is needed can be as effectively achieved in a way that is less restrictive of the person’s rights and freedom of action.
2. People who lack capacity (1) For the purposes of this Act, a person lacks capacity in relation to a matter if at the material time he is unable to make a decision for himself in relation to the matter because of an impairment of, or a disturbance in the functioning of, the mind or brain. (2) It does not matter whether the impairment or disturbance is permanent or temporary. (3),4), 5) […]
Inability to make decisions(1) For the purposes of section 2, a person is unable to make a decision for himself if he is unable – (a) to understand the information relevant to the decision (b) to retain that information (c) to use or weigh that information as part of the process of making the decision, or (d) to communicate his decision (whether by talking, using sign language or any other means).(2) The fact that a person is able to retain the information relevant to a decision for a short period only does not prevent him from being regarded as able to make the decision.(3) The information relevant to a decision includes information about the reasonably foreseeable consequences of – (a) deciding one way or the other, or (b) failing to make the decision
4 Best interests (1) In determining for the purposes of this Act what is in a person’s best interests, the person making the determination must not make it merely on the basis of - (a) the person’s age or appearance, or (b) a condition of his or an aspect of his behaviour which might lead others to make unjustified assumptions about what might be in his best interests. (2) The person making the determination must consider all the relevant circumstances and, in particular, take the following steps. (3) He must consider— (a) whether it is likely that the person will at some time have capacity in relation to the matter in question, and (b) if it appears likely that he will, when that is likely to be. (4) He must, so far as reasonably practicable, permit and encourage the person to participate, or to improve his ability to participate, as fully as possible in any act done for him and any decision affecting him. (5)Where the determination relates to life-sustaining treatment he must not, in considering whether the treatment is in the best interests of the person concerned be motivated by a desire to bring about his death. (6) He must consider, so far as is reasonably ascertainable— (a) the person’s past and present wishes and feelings, (b) the beliefs and values that would be likely to influence his decision if he had capacity, and (c) the other factors that he would be likely to consider if he were able to do so.
(7) He must take into account, if it is practicable and appropriate to consult them, the views of – • anyone named by the person as being someone to be consulted on the matter in question or on matters of that kind • Anyone engaged in caring for the person or interested in his welfare • Any donee of a lasting power of attorney granted by the person, and • Any deputy appointed for the person by the court • as to what would be in the person’s best interests and, in particular, as to the matters mentioned in subsection (6). • (8) The duties imposed by subsections (1) to (7) also apply in relation to the exercise of any powers which— • (a) are exercisable under a lasting power of attorney, or • (b) are exercisable by a person under this Act where he reasonably believes that another person lacks capacity. • (9) In the case of an act done, or a decision made, by a person other than the court, there is sufficient compliance with this section if (having complied with the requirements of subsections (1) to (7)) he reasonably believes that what he does or decides is in the best interests of the person concerned.
Best Interests (s.4) • Need to consider:- • Is the person likely to regain capacity & when? • Maximise participation in process • Past and present wishes of person • Their beliefs, values and other factors • Views of carers and other nominated or appointed persons
Acts in connection with care or treatment (s.5) • “(1) If a person (‘D’) does an act in relation to care or treatment of another person (‘P’), the act is one to which this section applies, if: • (a) before doing the act D takes reasonable steps to establish whether P lacks capacity in relation to the matter in question, and • (b) when doing the act, D reasonably believes (i) that P lacks capacity in relation to the matter (ii) that it will be in P’s best interests for the act to be done.”
Acts in connection with care or treatment (s.5) • “(2) D does not incur any liability in relation to the act that he would not have incurred if P - (a) had had the capacity to consent in relation to the matter (b) had consented to D’s doing the act.” • (3) […] • (4) […]
s.6 – s.5 acts: limitations • (1) If D does an act that is intended to restrain P it is not an act to which s.5 applies unless two further conditions are satisfied. • (2) The first condition is that D reasonably believes that it is necessary to do the act to prevent harm to P
s.6 – s.5 acts: limitations • (3) The second is that the act is a proportionate response to - • (a) the likelihood of P’ suffering harm • (b) the seriousness of the harm • (4) For the purposes of this section D restrains P if he – • (a) uses, or threatens to use, force to secure the doing of an act which P resists, or • (b) restricts P’s liberty of movement whether or not P resists.
s.6 – s.5 acts: limitations • (5) But D does more than merely restrain P if he deprives P of his liberty within the meaning of Article 5(1) of the ECHR (whether or not P is a public authority).
Kerrie Wooltorton 1981-2007 • Died 19-09-07 from ethylene glycol poisoning • Detained s.3 MHA March 2009. Diagnosed with emotionally unstable personality disorder • 14-09-07 wrote letter declining life saving treatment • Did not lose capacity during treatment
Mental Capacity Act 2005 (2) • s.9 Lasting Powers of Attorney • s.15 Power to make declarations • s.16 Power to appoint deputies • s.17/18 Powers of the Court • s.24-26 Advance Decisions • s.28 Mental Health Act Matters
Advance decisions to refuse treatment MCA Code para 9.10 - 11 • There are no formalities about the format of an AD unless it deals with life-sustaining treatment • Must state precisely what treatment is to be refused • May set out circumstances • Will only apply when P lacks capacity
What is an Advance Decision? MCA s.24 (1) “Advance decision” means a decision made by a person (“P”), after he has reached 18 and when he has capacity to do so, that if— (a) at a later time and in such circumstances as he may specify, a specified treatment is proposed to be carried out or continued by a person providing health care for him, and (b) at that time he lacks capacity to consent to the carrying out or continuation of the treatment, the specified treatment is not to be carried out or continued.
Effect of ADs (MCA s.26(2-3)) (2) A person does not incur liability for carrying out or continuing the treatment unless, at the time, he is satisfied that an advance decision exists which is valid and applicable to the treatment. (3) A person does not incur liability for the consequences of withholding or withdrawing a treatment from P if, at the time, he reasonably believes that an advance decision exists which is valid and applicable to the treatment.
Awareness of ADs (MCA Code) • “It is the responsibility of the person making the advance decision to make sure their decision will be drawn to the attention of healthcare professionals when it is needed”
Mental Capacity Act 2005 (3) • s.30 Research • s.35-41 Independent Advocates (IMCAs) • s.37 Duty to seek advice in connection with serious medical treatment • s.38 Duty of NHS bodies to seek advice before placement • s.39 Duty of local authority to seek advice before placement
Mental Capacity Act 2005 (4) • s.42 Code of Practice Research • s.44 Ill treatment or neglect • s.45 Court of Protection • s.57 Public Guardian • s.61 Court of Protection Visitors • Sch A1 Deprivation of Liberty
Code of Practice Published February 2007 302 pages
Deputies Attorneys Research workers IMCAs Doctors Nurses Solicitors Physiotherapists OTs Social Workers Community Care Assistants Family members “Good Samaritans” All of the above Who has to know about the Code of Practice?
IMCA • Provision of serious medical treatment • Provision of accommodation by NHS • Provision of accommodation by LA • Adult protection • Bournewood
Vulnerable adults • A vulnerable adult is a person aged 18 years or over who may be unable to take care of themselves, or protect themselves from harm or from being exploited. This may be because they have a mental health problem, a disability, a sensory impairment, are old and frail, or have some form of illness.
Lasting Power of Attorney • Two forms for • 1. Property and affairs • 2. Health and Welfare • Certificate of capacity • LPAs will have to be registered before use • Register will be accessible – a) general b) specific
LPAs • “Although the PG will maintain a register of LPAs, in practice, the OPG will carry out little or no supervision or monitoring of these cases, beyond ensuring that the registration process prescribed by the Act is properly followed.”
Code of Practice • s. 42 (4) It is the duty of a person to have regard to any relevant code if he is acting in relation to a person who lacks capacity and is doing so in one or more of the following ways- (a) as the donee of a lasting power of attorney, (b) as a deputy appointed by the court, (c) as a person carrying out research in reliance on any provision made by or under this Act (see sections 30 to 34), (d) as an independent mental capacity advocate, (e) in a professional capacity, (f) for remuneration.
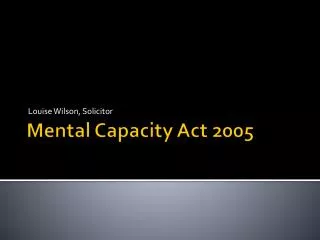
Overview of Deprivation of Liberty Safeguards Proposals A) Hospital or care home managers identify those at risk of deprivation of liberty and request authorisation from supervisory body In an emergency hospital or care home can issue an urgent authorisation for seven days while obtaining authorisation B) Assessment commissioned by supervisory body. IMCA instructed for anyone without representation Age assessment No refusals assessment Eligibility assessment Mental health assessment Mental capacity assessment Best interests assessment Authorisation expires and managing authority requests further authorisation All assessments support authorisation Any assessment says no E) Best interests assessor recommends person to be appointed as representative D) Best interests assessor recommends period for which deprivation of liberty should be authorised C) Request for authorisation declined F) Authorisation is granted and person’s representative appointed Person or their representative appeals to Court of Protection which has powers to terminate authorisation or vary conditions G) Authorisation implemented by managing authority Briefing sheet – Deprivation of Liberty Safeguards – November 2007 Gateway reference: 8965 Managing authority requests review because circumstances change Person or their representative requests review 42 H) Review
What isn’t covered in MCA • consent to sexual conduct • consent to place children for adoption • consent to marriage/civil partnership • ‘no fault’ divorce • parental responsibilities other than those related to property • voting
Deal with finances Make a will Make a Gift Enter litigation Contract Vote Enter personal relationships Consent to and refuse medical treatment Consent to research and innovative treatment NOT decide where to live Specific tests of capacity
Further reading Blackstone’s Guide to the Mental Capacity Act P Bartlett (2005) Oxford University Press