Download
1 / 29
300 likes | 755 Views
CHAPTER 14. Psychological Disorders Schizophrenia. Schizophrenia. Schizophrenia is a disabling disorder characterized by perceptual disturbances Emotional disturbances intellectual deficits loss of contact with reality Often an inability to function in life. Incidence rate:

E N D
CHAPTER 14 Psychological Disorders Schizophrenia
Schizophrenia • Schizophrenia is a disabling disorder characterized by • perceptual disturbances • Emotional disturbances • intellectual deficits • loss of contact with reality • Often an inability to function in life. • Incidence rate: • estimated that 3 million Americans will develop schizophrenia during their lifetime. • Approximately 2% of population • 100,000 patients take up 20% of psychiatric beds in the U.S. • Many more receive outpatient care.
Schizophrenia • Term “schizophrenia” first coined in 1911: • Swiss psychiatrist EugenBleuler • combination of two Greek words meaning “split mind.” • refers to the distortion of thought and emotion, which are “split off” from reality • NOT split personality (and you get an F if you define it as that on the test!). • Schizophrenia is a psychosis: individual has severe disturbances of • reality • orientation • thinking
Diagnosing Schizophrenia • Must exhibit some combination of several symptoms: • Hallucinations : • internally generated perceptual experiences • E.g., voices telling the person what to do. • Delusion : • false, unfounded beliefs, • such as that one is a messenger from God. • Paranoia: characterized by delusions of persecution. • Disordered thought: • Lack of logic in thought processes • Word salad or fleeting thoughts • Inappropriate emotions or lack of emotion • Social withdrawal.
Schizophrenia • Schizophrenia often subdivided into diagnostic categories • based on which of these symptoms is predominant • May include • Paranoid • Hebaphrenic • Undifferentiated • Catatonic. • Researchers disagree: about relatedness of schizophrenia and some other disorders • Are some personality disorders sub-types of schizophrenia • May be related spectrum disorders • E.g., schizotypal personality or schizoid personality
Etiology • No gender difference: • Schizophrenia afflicts men and women about equally often. • Men usually show the first symptoms during the teens or twenties, • Onset for women ordinarily comes about a decade later. • Acute symptoms: • Typically develop suddenly • typically more responsive to treatment. • The prognosis is reasonably good in spite of brief relapses. • Chronic symptoms • Symptoms that develop gradually • persist for a long time with poor prognosis • What do symptoms “feel” like? • http://www.youtube.com/watch?v=kvdw4b7tC-8
Positive vs. negative symptoms • Positive symptoms • Involve the presence or exaggeration of behaviors • Include • delusions • hallucinations • thought disorder • bizarre behavior • Negative symptoms • characterized by the absence or insufficiency of normal behaviors • include • lack of affect (emotion) • inability to experience pleasure • lack of motivation • poverty of speech • impaired attention.
etiology • Schizophrenia is a familial disorder: • incidence of schizophrenia higher among the relatives of schizophrenics than in general population. • Identical twins of schizophrenics are three times as likely to be schizophrenic as the fraternal twins of schizophrenics. • The heritability for schizophrenia has been estimated at between .60 and .90. • This means that 10-40% of the variability is due to environmental factors.
Schizophrenia • Adoption studies • Results from adoption studies gives more impressive indication of genetic influence. • adopting out of a schizophrenic home provides little or no protection from schizophrenia. • No difference in rate of schizophrenia between adopted or reared by biological parents • Interesting: percentage of individuals affected relatively stable cross-culturally • Further supports hypothesis that it is a genetic disorder
Schizophrenia • Researchers made significant progress in understanding genetic influences • identified a handful of genes responsible for schizophrenia • reasonably good assurance that genes are correctly identified. • The genes primarily concerned with • neuronal migration, • neuroreceptor development or sensitivity • neurotransmitter activity. • teasing out the genes’ relationships to behavioral symptoms. • Vulnerability model: • Some threshold of causal forces must be exceeded in order for illness to occur. • Environmental challenges combine with person’s genetic vulnerability to exceed that threshold. • Genes determine only vulnerability for illness, not actual disease progression • Both heredity and environment needed to explain the etiology (causes) of schizophrenia.
History of treatment • Early 20th century: • Little could be done to treat psychotic patients until mid-1950s • In mid 1950’s: variety of antipsychotic medications arrived on the scene. • Anitpsychotics not originally designed to treat schizophrenia • often is case in medicine • Most often in mental health • researchers had too little understanding of the disease to develop specific meds • Tried horse tranquilizers, brain surgeries, other wild treatments • Chlorpromazine or Thorazine: • Tried with wide variety of mental illnesses • Used it because it calmed surgical patients (and horses) • Found it reduced schizophrenia symptoms • NOT clear why chlorpromazine worked, • Traditional tranquilizers have little or no usefulness in treating schizophrenia. • Only Thorazine seemed to calm these patients
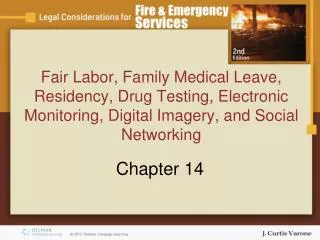
Amphetamine hypothesis • Amphetamine • overdose causes psychotic behavior indistinguishable from schizophrenia, • Includes symptoms such as hallucinations and paranoid delusions. • Dopamine Hypothesis • Researchers determined that amphetamine produces these symptoms by increasing dopaminergic activity • eventually led to the dopamine hypothesis • schizophrenia involves excessive dopamine activity in the brain. • blockade of type D2 dopamine receptors is essential for a drug to have an antipsychotic effect, • effectiveness directly related to drug’s D2 receptor blocking potency.
The horizontal axis: average daily doses prescribed by physicians Horizontal red lines represent typical ranges of doses. Values on vertical axis are amounts of drug required to block 50% of the dopamine receptors.
Schizophrenia • Tardive Dyskinesia • Prolonged use of antidopamine drugs often produces • Includes permanent tremors and involuntary movements caused by blocking of dopamine receptors in the basal ganglia. • Pill rolling, grimacing, etc. • http://www.youtube.com/watch?v=BJjXqKa4cbE • http://www.youtube.com/watch?v=HEKxWzvoD7M • The effect appears to be due to a compensatory increase in the sensitivity of D2 receptors in the basal ganglia.
Schizophrenia • Atypical antipsychotics • Risperidal; Olazapine, etc. • Introduced in early 1990s • are referred to as atypical because work slightly differently than original D2 antagonists. • How are they different? • Less specifically target D2 receptors • produce motor problems only at much higher doses • Later onset of motor problems • Major side effects, particularly on white blood cells. • Some suggest atypical antipsychotics are 15-25% more effective than conventional antipsychotics; data NOT support this. • Although target receptors other than the D2, those that lack at least a modest effect at D2 receptors are therapeutically ineffective.
Schizophrenia symptoms occur elsewhere • Phencyclidine (PCP): • elicits some of the symptoms of schizophrenia • mimics schizophrenia better than amphetamine does. • PCP inhibits the NMDA glutamate receptor • suggests that reduced glutamate might be a factor in schizophrenia. • Glutamate theory: • reduced glutamate activity involved in schizophrenia • Strong theoretical and therapeutic promise with this theory. • The glutamate system influences number of dopamine receptors. • Atypical antipsychotics also affect the serotonin system, which helps regulate the dopamine system.
Brain changes in Schizophrenia • Several changes in brain of individuals with Schizophrenia • reduced cortical gray matter • reduced limbic area volume • enlarged fissures and sulci • enlarged ventricles in the brains of schizophrenics. • Deficits are often accompanied by enlarged ventricles. • Ventricular enlargement serves as a marker or indicator of the tissue deficiency • ventricles expand to take up space normally occupied by brain cells • Suggests actual neuronal loss • Degree of ventriclar enlargement correlated with decrease in IQ. .
Brain changes in Schizophrenia • Are deficits due to loss of specific area or coordination of several areas? • Recent research: suggest schizophrenia due to disordered connections between parts of the brain • Not due to localized malfunction. • This consistent with findings of reduced white matter in the brains of schizophrenics. • Remember: White matter= axons • Reduction not due to loss of neurons themselves, but loss of connections between neurons • Do connections die, resulting in symptoms? • Do symptoms produce loss of neurons?
Changes in cognitive function • Many schizophrenics perform poorly on the Wisconsin Card Sorting Task • Wisconsin Card sorting Task • Sort cards by color, shape, symbol • Have subject switch to new type of sorting across several trials • Requires the individual to switch from one card sorting strategy to another. • Many schizophrenics perform poorly on the test, persisting with the previous sorting strategy.
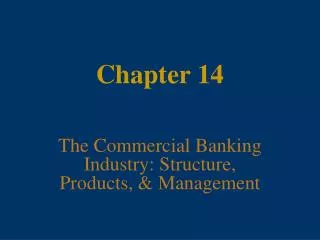
Changes in cognitive function • Poor performance on Wisconsin Sorting Task suggests poor prefrontal activity • Normal individuals: increased activation in the prefrontal area during the test • Schizophrenics do not. • This hypofrontality appears to involves DA deficiency • administering amphetamine to schizophrenics increases blood flow in the prefrontal cortex • Amphetamine also improves performance on the Wisconsin Card Sorting Task. • Question is why DA decreases!
Blood flow in normal and schizophrenic brains during card sorting test (a) The upper images are of the left and right hemispheres of a normal brain; the schizophrenic brain is below. Red and yellow represent greatest activation. (b) Note Activity in the dorsolateral prefrontal cortex, whose location is identified figure to right, appears most compromised.
Why the damage? • Some of the brain defects in schizophrenia apparently stem from problems during pregnancy or at the time of birth. • Prenatal problems include • physical complications of mother and fetus • emotional stresses on the mother. • birth and pregnancy complications associated with • brain deficits • enlarged ventricles later in life.
Why the damage? • Winter effect: • more schizophrenics are born during the winter and spring than during any other time of the year. • Infants born between January and May • experienced second trimester of prenatal development in the fall or early winter: • high incidence of infectious diseases. • Strong evidence that the mother’s exposure to viral infections during the 4th-6th months of pregnancy increases risk of schizophrenia. • Prenatal starvation is another pathway to schizophrenia. • Poor maternal diet • Issues with metabolizing across placenta
Why the damage? • Bottom line: • Schizophrenia may include predisposition of some kind • May be related to autoimmune function • May result in changes in axonal growth/brain development, particularly in ventricles