Download
1 / 42
430 likes | 724 Views
Orthomyxoviruses (Influenza virus). 25 Muharram 1428H 13 Feb 2007 SBM 2044. In 1918 children would skip rope to the rhyme*: I had a little bird, Its name was Enza. I opened the window, And in-flu-enza.

E N D
Orthomyxoviruses (Influenza virus) 25 Muharram 1428H 13 Feb 2007 SBM 2044
In 1918 children would skip rope to the rhyme*: I had a little bird, Its name was Enza. I opened the window, And in-flu-enza. * Taken from Crawford, Richard, "The Spanish Flu," Stranger Than Fiction: Vignettes of San Diego History San Diego Historical Society, 1995
The influenza pandemic of 1918-1919 killed more people than the World War I (WWI), at somewhere between 50 and 100 million people. This was caused by the deadly strain subtype H1N1 influenza type A virus. It has been cited as the most devastating epidemic in recorded world history. More people died of influenza in a single year than in four-years of the Black Death Bubonic Plague from 1347 to 1351.
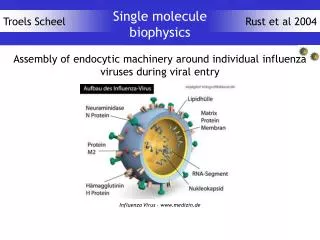
Orthomyxoviruses • Major cause of respiratory disease. Influenza (flu) can cause mild to severe illness, and has been responsible for millions of deaths worldwide. • ss negative-sense RNA. The antisense RNA genome occurs in eight separate segments containing 10 genes. • The envelope contains viral haemagglutinin (HA) and neuraminidase (NA) proteins. • Genetic reassortment of Influenzavirus is common. The segmented viral genome allows a mixture of genome segments from two strains, when a single cell is infected by 2 different strains.
Classification • Antigenic differences exhibited by two of the internal structural proteins: nucleocapsid (NP) and matrix (M) proteins, are used to divide influenza viruses into types AC. NP antigens are stable and exhibit no serologic cross reactivity. • Surface glycoproteins: HA and NA, are used to subtype the viruses. These two antigens are variable. These Ags are responsible for immunity to infection. • So far, 15 subtypes for HA (H1-H15); and 9 subtypes for NA (N1-N9) have been recovered from birds, animals and humans. • In humans, there are 4 HA (H1-3,H5) and 2 NA (N1-2).
Function of HA • Haemagglutinin = agglutinate erythrocytes under certain conditions. • HA binds virus particles to susceptible cells, and is the major Ag against neutralising Abs.
Function of NA • Functions at the end of viral replication cycle. It is a sialidase that removes sialic acid from glycoconjugates. • Facilitates release of virus particles from infected cell surfaces during the budding process. And prevent self-aggregation of virions by removing sialic acid residues from viral glycoproteins. Also may help the virus to slide through the mucin layer in resp T to reach the target epithelial cells.
Influenza virus ReplicationExpert Reviews in Molecular Medicine 2001 Cambridge University Press
(a) The virus binds to cell-surface sialic acid receptors on the surface of the host cell and (b) is internalised into endosomes, by receptor-mediated encytosis. (c) Fusion btw viral envelope and cell membrane, and uncoating events, (d) Low pH is required by the virus-mediated membrane fusion to release of the viral genome (RNPs) into the cytoplasm. The vRNPs are then imported into the nucleus for (e) replication. (f) mRNAs are produced from viral nucleocapsids. Positive-sense viral messenger RNAs (mRNAs) are exported out of the nucleus into the cytoplasm for (g) protein synthesis. Cellular functions are more involved. Protein synthesis requires cellular transcripts and RNA polymerase II, which explains why influenza virus is inhibited by drugs that block cellular transcription. (h) Some of the proteins are imported into the nucleus to assist in viral RNA replication and (i) vRNP assembly, which also occur in the nucleus. (j) Late in infection, the vRNPs form and leave the nucleus, and (k) progeny viruses assemble and (l) bud from the plasma membrane. • The sites of action of anti-viral drugs are shown in red, italic text. Abbreviations used: cRNA (+), positive-sense complementary RNA; HA, haemagglutinin; M1, matrix protein; M2, tetrameric ion channel; mRNA (+), positive-sense messenger RNA; NA, neuraminidase; NP, nucleoprotein; NS1, a non-structural protein, NS2, a viral protein; pols, polymerases; vRNA (-), negative-sense genomic RNA
Pathogenesis & Pathology • Spreads from person to person by airborne droplets, or contaminated hands and surfaces. • Viral NA lowers the viscosity of the mucous film in the resp T, exposing the cellular surface receptors and promoting the spread of virus-containing fluid to lower resp T. Within short time, many resp cells are infected and eventually killed. • Interferon is effective against influenza virus and attributes to host recovery. • Influenza infections cause cellular destruction and desquamation of superficial mucosa of the respiratory tract but do not affect the basal layer of epithelium. Viral damage in the epith lowers its resistance to secondary bacterial invaders esp staphylococci, streptococci and Haemophilus influenzae.
Antigenic Drift & Shift • Antigenic variants confer selective advantage over the parental virus in the presence of Ab against the original strain. • The 2 surface Ags undergo antigenic variation independent of each other. • Antigenic drift = Minor changes, a gradual change in antigenicity due to point mutations that affect major antigenic sites on the glycoprotein. • Antigenic shift = Major changes, an abrupt change due to genetic reassortment with an unrelated strain, which results in the appearance of a new subtype.
Clinical findings • Uncomplicated Influenza : Abrupt symptoms include chills, headache, dry cough, muscular aches. These may be induced by influenza A or B. In contrast, influenza C causes a common cold illness, Coryza. • Pneumonia : complications occur only in the elderly and debilitated. Influenza infection enhances the susceptibility of patients to bacterial superinfection, due to loss of ciliary clearance, dysfunction of phagocytic cells. • Reye’s Syndrome : an acute encephalopathy of children and adolescents (2-16yrs)
Immunity • Is long-lived and subtype specific. • Abs to HA and NA are important. Resistance to initiation of infection is related to Ab vs. HA, whereas severity of disease and ability to transmit virus to contacts are associated with Abs vs. NA. • Local secretory IgA Abs is probably important in preventing infection. Serum Abs are also protective and persist for years. Abs modify the course of illness – person with low titres of Abs may experience mild form of illness. • Cell-mediated immune response is probably important for clearance of an infection. Cytotoxic T lymphocyte response is cross-reactive ie. able to lyse cells infected by any subtype of virus, and is directed against both internal proteins (NP, M) and the surface glycoproteins.
Epidemiology • Periodic outbreaks appear because of antigenic changes in one or both surface glycoproteins of the virus. • Only influenza A viruses circulate in animals and avians. Antigenic shift ? • The recent strain in avian influenza A virus (H5N1) in 1997, reported in Hong Kong. The source was domestic poultry. At present, there is no vaccine against this strain.
Prevention & Control by Vaccines • A) Inactivated Viral Vaccines: • Parenteral use;usually contain 1 or 2 type A and a type B viruses, isolated from previous winter’s outbreaks. • Strains are grown in embryonated eggs and the virus is harvested from egg allantoic fluid. • Vaccines are either whole virus (WV), subvirion (SV), or surface Ag (SAg) preparations. WV=contains intact, inactivated virus; SV=purified virus disrupted with detergents; SAg contains purified HA and NA glycoproteins. • Sometimes called “flu shot” or “flu jab”.
Prevention & Control by Vaccines • B) Live Attenuated Influenza Vaccine • Contains live but attenuated (weakened) vaccine. It is sprayed into nostril. • For both types of vaccines, it will take up to 2 weeks to develop protection after vaccination. • The synthetic drugs amantadine and rimantadine hydrochloride effectively prevent infection and illness caused by type A, but not by type B, viruses. The drugs interfere with virus uncoating and transport by blocking the transmembrane M2 ion channel (see fig of replication).
Paramyxoviruses 25 Muharram 1428H 13 Feb 2007 SBM 2044
Paramyxoviruses • The World Health Organisation (WHO) estimates that acute respiratory infections and pneumonia are responsible every year worlwide for the deaths of 4 million children under 5 years of age. • Paramyxoviruses are the major respiratory pathogens in this age group. • Reinfections are common throughout childhood. • All members of the Paramyxoviridae family initiate infection via the resp T. • Transmission is by person-to-person contact or by large-droplet aerosols.
General Structure • Enveloped. Viral genome is linear, negative sense ss RNA. Non-segmented genome, hence all members are antigenically stable. • Haemagglutinin glycoprotein HN proteins are important for viral attachment.
Pathogenesis of Parainfluenza Infections • Parainfluenza virus replication in immunocompromised appears to be limited to respiratory epithelia. Viraemia is rare. The result is “common cold” syndrome. • Infection may spread to larynx and upper trachea, resulting in croup. Croup is characterised by resp obstruction due to swelling of larynx and related structures. • Viral shedding is about 1 week after onset of illness. Some immunocompromised children experience persistent shedding.
Clinical findings & Lab diagnosis • Primary infections in children usually result in rhinitis, pharyngitis, often with fever. • Severe illness associated with Parainfluenza Type 3 may occur in infants. • Common complication is otitis media. • Lab: Ag detection – immunofluorescence test; isolation of virus-containing specimens; and serological by detecting specific IgM Ab. • Parainfluenza viruses are troublesome in hospitals. Contact isolation is necessary to prevent outbreaks. • Antiviral ribavirin is used to treat immunocompromised with lower resp T disease.
Respiratory Syncytial Virus • Most important cause of lower resp T illness in infants and young children. • Replication occurs initially in epithelial cells of the nasopharynx. Virus may spread into the lower resp T and cause bronchiolitis and pneumonia. • The incubation period between exposure and onset of illness is 3-5 days. • Viral shedding may persist 1-3 weeks in children; and 1-2 days only in adults. • RSV initially replicates in epithelial cells of nasopharynx, which then migrates to the lower resp T and causes bronchiolitis and pneumonia. The virus spreads both extracellularly and by fusion of cells to form syncytia.
Treatment • Treatment on supportive care (eg. removal of secretions, administration of O2) • A promising means of protection is the administration of RSV-enriched polyclonal immunoglobulin (RSVIG) with monthly high-dose infusion. The maintenance of high-titer RSV neutralizing antibodies seems to significantly decrease the incidence and severity of respiratory syncytial virus illness in children at high risk. • Ribavirin – in the US. • As yet, there is no safe and effective vaccine against RSV.
Mumps Virus • Is an acute contagious disease characterised by non-suppurative enlargement of one or both salivary glands. • Mostly causes mild childhood disease, but in adults, complications inc meningitis and orchitis are common. • More than 1/3 of mumps infections are asymptomatic, but equally capable of transmitting the virus. • Humans are the only natural hosts.
Pathogenesis & Pathology • Primary replication occurs in nasal and upper resp T epithelial cells viraemia salivary G & other organs (NB. Parotid G is not compulsory) • Incubation period may range from 2-4 wks. • Virus shed in saliva from about 2 days before to 9 days after the onset of salivary G swelling. • It is difficult to control transmission since mumps is asymptomatic and has a variable incubation periods. • Virus frequently infects kidneys, detectable in urine. CNS is commonly infected and may be involved in the absence of parotitis. • Testes and ovaries may be affected, esp after puberty. 20-50% of males infected with mumps virus develop orchitis, and lack elasticity of the tunica albuginea which prevents testis to swell. This results in pressure necrosis, but rarely results in sterility. 5 % of women develops mumps oophoritis.
Immunity vs. Mumps Virus • Immunity is permanent after a single infection. • Only one antigenic type of mumps virus. • Abs develop against surface glycoproteins and internal nucleocapsid protein. • Interferon induced early in mumps infection. IgA secreted in nasopharynx. • Passive immunity from motheroffspring. Hence, rare mumps in infants < 6 mth.
Diagnosis • Mumps virus is isolated from saliva, CSF, urine. • Serology: detect mumps-specific IgM or IgG. • Mumps primarily is an infection of children 5-9 yrs is the highest incidence. • Transmission by close contact eg. Crowded areas (army camps).
Treatment • No specific therapy. • Immunisation with attenuated live mumps virus vaccine to reducing mumps-associated morbidity and mortality. • Isolation of infected subjects to prevent outbreak. • Mumps vaccine available in MMR (mumps, measles and rubella). Produce Abs to each viruses in ~95% vaccinees.
Histological diagnosis: Haemadsorption by Mumps virus Large syncytia by Respiratory Syncytial virus
Measles (Rubeola) Virus • Measles is an acute, highly infectious disease characterised by fever, resp symptoms and maculopapular rash. • Complications are common. • Although there is a vaccine, incidence is low, but still a leading cause of death in young children in developing countries. • Humans are the only host. Other animals can be experimentally infected.
Pathogenesis & Pathology Virus enters resp T (and multiply locally) Lymphoid tissues (more multiplication) 1° viraemia Reticuloendothelial 2° viraemia epithelial surface Skin resp T conjunctiva Aids dissemination throughout body - seen as multinucleated giant cells
Pathogenesis • Rash appears at about day 14, just as circulating Ab is detectable, viraemia disappears and fever falls. Rash develops as a result of interaction of immune T cells with virus-infected cells in the small blood vessels and lasts about 1 week. (Thus, patients with defective cell-mediated immunity will have no rash) • Brain/CNS infection is common. Complication subacute sclerosing panencephalitis that develops years after infection, caused by viruses remaining in the body. • Viral replication is defective owing to the lack of production of one or more viral gene products, often matrix protein.
Clinical Findings • Fever, sneezing, coughing, running nose and redness of eyes; Koplik’s spots (small bluish-white ulcerations on the buccal mucosa opposite lower molars) and lymphopenia. • Rash starts on head, spreads to the chest, trunk, lower limbs. • Pneumonia – most common life-threatening complications of measles, by 2° bacterial infections. • More serious complications acute encephalitis • Subacute sclerosing panencephalitis occur insidiously 5-15 yrs after case of measles, characterised by progressive mental deterioration, involuntary movements, muscular rigidity and coma.
Immunity • There is only one antigenic type, hence infection confers lifelong immunity. • Patients with Ig-defective recover well, whereas cellular immune-deficiency do poorly. • Abs to nucleoprotein is the most useful – the most abundant viral protein in cells.
Epidemiology and Treatment • Transmission is predominantly via resp route. Haematogenous transplacental transmission during pregnancy. • Continuous supply of susceptible individuals is required for the virus to persist in a community. • Measles is endemic worldwide. Epidemics recur regularly every 2-3 years. • Rx: live attenuated measles virus vaccine (monovalent or combination with rubella – MMR). • Vaccinees may experience mild clinical reactions, but no virus excretion and no transmission.
Nipah Virus & Hendra Virus • Zoonotic paramyxoviruses. • 1998-99: severe encephalitis in Malaysia by Nipah virus. High mortality rate up to 70%. Infection caused by direct viral transmission from pigs to humans. • Hendra virus is an equine virus. • Fruit bats (flying foxes) are natural hosts for both Nipah and Hendra viruses. • Ecologic changes inc land use and animal husbandry practices are probably the reason for the emergence of these two infectious diseases.
Rubella/German Measles • Is an acute febrile illness characterised by a rash and lymphadenopathy that affects children and young adults. A self-limiting illness. • It is the mildest of common viral exanthems but infection during early pregnancy may results in congenital malformations and mental retardation. • Rubella virus is a member of Togaviridae.
Postnatal Rubella • Neonatal, children and adults may be infected whereby infections starts in upper resp T, and multiplication in cervical lymph nodes viraemia. • Fever, malaise and a morbiliform rash. Rash starts on face, extends over trunk and extremities. But rarely lasts more than 3 days. • Lab diagnosis is unreliable because similar symptoms are seen with other viruses.
Congenital Rubella • Occurs when maternal viraemia placenta and foetus • In infected foetus, growth rate is reduced, results in deranged/hypoplastic organ development. The earlier in the pregnancy infection occurs, the greater the damage to the foetus. • Newborn will have cardiac abnormalities, deafness, rash, hepatosplenomegaly and jaundice. Rubella panencephalitis (rare) in second decade of life. • Immunity: IgG = maternal rubella Ab which lost after 6mths; IgM = diagnostic of congenital rubella, since IgM does not cross placenta, so its presence concurs the IgM synthesis by infants in utero. • Rx: No specific treatment. Best to prevent the disease.