Download
1 / 28
280 likes | 469 Views
Preparazione farmacologica alla PTCA: trattamento antiaggregante/anticoagulante precoce o in sala di emodinamica: il parere dell’ emodinamista C. Cavallini (Perugia). Aspirin in Percutaneous Coronary Interventions.

E N D
Preparazione farmacologica alla PTCA: trattamentoantiaggregante/anticoagulante precoce o in sala di emodinamica:il parere dell’emodinamistaC. Cavallini (Perugia)
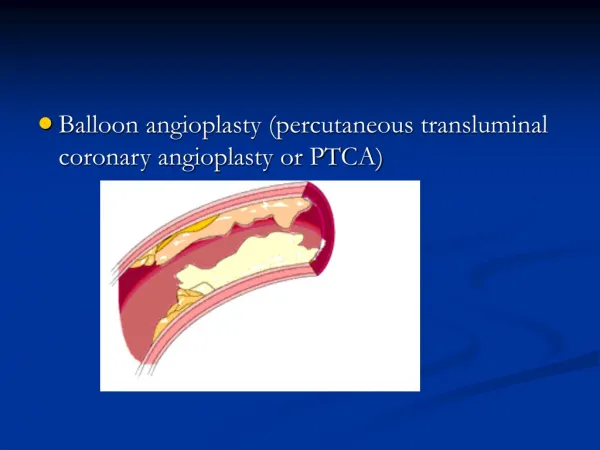
Aspirin in Percutaneous Coronary Interventions In the first reported percutaneous coronary intervention, 3 days of aspirin was empirically added to full anticoagulation with heparin. Gruentzig AR: N Engl J Med 1979;301:61
Risultati del pretrattamento con eparina nei candidati a PTCA con angina instabile Nessuno di questi studi era randomizzato; tuttavia i presupposti razionali, e la concordanza dei risultati portano all’unanime consenso di raccomandare il pre-trattamento con eparina per 48-72 ore nei pazienti più instabili prima di procedere all’angioplastica coronarica. Cavallini, Atti convegno De Gasperis, Milano 1997
Farmaci antitrombotici e NSTEMI Prasugrel Clopidogrel Eptifibatide Tirofiban ASA LMWH UFH Abciximab Fundaparinux Bivalirudina
Quale Anticoagulante ? • UFH • LMWH • Fundaparinux • Bivalirudina Cosa Chiede l’Emodinamista 1) Effetto dose/risposta prevedibile 2) Breve Emivita (rimozione introduttore) 3) Efficacia antitrombotica (anche su trombosi catetere) 3) Basso tasso di complicanze emorragiche
Anticoagulant therapy for an urgent invasive approach ESC ACC/AHA ____________________________________________ UFH IC IA Enoxaparin IIa-B IA Fondaparinux IB Bivalirudin IB IB
STEEPLE Trial: Secondary Endpoint Analysis of patients reaching target anticoagulation levels at the start and end of procedure (%) p<0.001 vs UFH p<0.001 vs UFH • The percent of patients reaching target anticoagulation levels at the start and end of the procedure was significantly lower among the UFH treatment group compared with the two enoxaparin treatment groups (78.8%, 91.7% vs 19.7%) Presented at ESC 2005
OASIS-5 PCI: Enoxaparin - Abrupt closure or threatened abrupt closure - P=0.026 Enoxa alone UFH+ Enoxa Mehta SR et al., J Am Coll Cardiol 2007
L’inibizione selettiva del fattore Xaproduce un effetto altamente prevedibile sulla formazione di trombina Fondaparinux: Profilo Farmacologico Farmacocinetica Inibizione lineare e dose-dipendente della formazione ex vivo di trombina in plasma umano povero di piastrine 70 60 50 40 Inibizionedellaformazione ditrombina (%) 30 20 10 0 0 1.5 3 4.5 6 7.5 Concentrazione di fondaparinux (µg/mL) Range terapeutico • Lormeau JC, HeraultVP.ThrombHaemost. 1995; 74(6):1474–1477
Major Bleeding: 9 Days Enoxaparin 0.04 HR 0.52 95% CI 0.44-0.61 P<0.00001 0.03 Cumulative Hazard 0.02 Fondaparinux 0.01 0.0 0 1 2 3 4 5 6 7 8 9 N Engl J Med 2006; 354, 1464-76 Days
Incidence (%) 10 P = 0.96 P = 0.39 P = 0.24 8.0 6.7 5 2.5 2.5 1.3 0 0 Abrupt closure Abrupt & threatened closure Abrupt & threatened closure, catheter thrombus OASIS-5 PCI: EnoxaparinvsFondaparinux - Wire Thrombosis- Enoxaparin (n = 80) Fondaparinux (n = 75) Mehta SR et al., J Am Coll Cardiol 2007
UFH/Enoxaparin+GPI (N=4603) Bivalirudin alone (N=4612) PNI <0.0001 PSup = 0.015 PNI = 0.011 PSup = 0.32 PNI <0.0001 PSup <0.0001 30 day events (%) 11,7% 10,1% 7,8% 7,3% 5,7% 3,0% Net clinical outcome Ischemic composite Major bleeding ACUITY Primary Endpoint Measures (ITT) UFH/Enoxaparin + GPI vs. Bivalirudin Alone Stone G ACC 06
ACUITY TRIAL • Not double blind trial • Non-inferiority margin issue • Low- Intermediate Risk profile • Major bleeding definition
Event rate in Major NSTE trial Low- to moderate risk event rate 30 D D/MI 30 D D/MI 30 D D/MI 30 D D/MI 30 D D/MI/ UR 30 D D/MI/ UR
ISAR-REACT-2 Primary Endpoint at 30 Days Composite of Death, MI or Urgent TVR Placebo (n=1010) Abciximab (n=1012) 20 Class 1A P=0.02; RRR:29% P=0.03 RRR:25% 16 18.3 13.1 11.9 12 % of Patients 8.9 8 4.6 4.6 4 0 Composite Whole Pop Composite Tp - Composite Tp + Kastrati A, et.al. JAMA 2006; 350 (3): 232-238.
If GP IIb/IIIablockerisneeded, • whentostart? • In the CCU (upstream) • in thecath-lab? (downstream)
50 Odds Ratio: 0.77 P=0.022 Odds Ratio 0.65 P=0.002 25.5% 40 25 Possible Partial Perfusion (TIMI 2) 20 18.1% 30 Possible Small Partial Perfusion (TIMI 2) 15 20 Small TIMI 1 10 Moderate % 10 24% Total Occlusion (TIMI 0) Moderate Total Occlusion (TIMI 0) 17% 5 Large 0 Large Occlusion Occlusion 0 Tirofiban + Heparin (n=570) Heparin (n=580) Tirofiban + Heparin (n=608) Heparin (n=622) PRISM-PLUS: Improvement in Thrombus Grade and TIMI Flow Grade with IIb/IIIa inhibition Zhao et al. Circulation 1999;100:1609-1615.
2 of 3 high-risk criteria: 1. Age > 60 years 2. + CKMB or TnT/I 3. ST or transient ST (Or age 50-59, h/o CVD and + CKMB or TnT/I) High-risk NSTE ACS n = 10,500 (9500) Early, routine eptifibatide (180/2/180) Placebo / provisional eptifibatide pre-PCI 39% of patients received eptifibatide during PCI Randomize within 12 hours of presentation Invasive strategy: 12 to 96 hours after randomization 1 Endpoint: 96-hr Death/MI/Urgent Revasc/Thrombotic bailout 2 Endpoint: 30-d Death/MI
15 N # Events Hours to Event Delayed provisional eptifibatide 4684 469 25.9 (18.7, 48.4) Early routine eptifibatide 4722 439 31.1 (18.8, 62.2) 10.0% 10 9.3% Delayed provisional eptifibatide Death, MI, RIUR or TBO (%) P = 0.23 (stratified for intended early clopidogrel use) 5 Early routine eptifibatide 0 0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96 Time Since Randomization (Hours) Primary Endpoint Giugliano, N Engl J Med 2009;360:2176-90.
Delayed Clinical Effect After Clopidogrel Loading Steinhubl SR et al., J Am Coll Cardiol 2006
Loading Dose and Variability of Platelet Aggregation Gurbel PA et al., J Am Coll Cardiol 2005
Clopidogrel: Double vs Standard Dose Primary Outcome: PCI Patients CV Death, MI or Stroke Clopidogrel Standard 15% RRR 0.04 Clopidogrel Double 0.03 Cumulative Hazard 0.02 HR 0.85 95% CI 0.74-0.99 P=0.036 0.01 0.0 0 3 6 9 12 15 18 21 24 27 30 Days
Farmaci antitrombotici e NSTEMI Prasugrel Clopidogrel Eptifibatide Tirofiban ASA LMWH UFH Abciximab Fundaparinux Bivalirudina
Ipotesi di utilizzo di Prasugrel nel paziente ACS-NSTE • Pz ad alto rischio in pre-trattamento con GPI e senza clopidogrel >coronarografia >Prasugrel 60/10 mg pre-PCI • Switch da clo a Prasugrel • Pz preloaded con 300/600mg Clop, PCI , switch a Prasugrel 10mg dopo la procedura. • >> in pazienti ad alto rischio ischemico/angiografico, o paz diabetici, o pazienti con eventi ricorrenti • Upstream in pazienti con scarsissima probabilità chirurgica (Pregresso CABG etc)
trattamentoantiaggregante/anticoagulante precoce o in sala di emodinamica:il parere dell’emodinamista • Trattamento precoce con anticoagulante: sempre • Quale anticoagulante: ...attendere prego! • Asa –Clo: sempre in pretrattamento (> 6 ore) • 2b/3a upstream? : pazienti molto instabili e con alta probabilità di CCH (no clopidogrel) • Prasugrel: no upstream, tranne STEMI