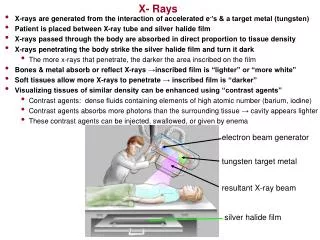
Download
1 / 43
550 likes | 1.18k Views
An approach to ankle x-rays. Aric Storck PGY2 (acknowledgement to Dr. Dave Dyck for several slides) September 11, 2003. Objectives. Review basic ankle fracture classification Review x-rays of common ankle fractures Discuss management of common ankle fractures. Case 1:. 25 year old female

E N D
An approach to ankle x-rays Aric Storck PGY2 (acknowledgement to Dr. Dave Dyck for several slides) September 11, 2003
Objectives • Review basic ankle fracture classification • Review x-rays of common ankle fractures • Discuss management of common ankle fractures
Case 1: • 25 year old female • Jumped off roof • Right ankle pain • Inability to weight bear on right foot • What else do you want to know on history and physical examination? • Does she need x-rays ?
Ottawa Ankle Rules: • Order ankle x-rays if acute trauma to ankle and one or more of • Age 55 or older • Inability to weight bear both immediately and in ER (4 steps) • Bony tenderness over posterior distal 6 cm of lateral or medial malleoli • Sensitivity ~100% • Specificity ~40%
You have decided to order an “ankle x-ray.” The nurse entering your orders asks which views you want …
Ankle X-rays: 3 views • AP • Identifies fractures of malleoli, distal tibia/fibula, plafond, talar dome, body and lateral process of talus, calcaneous • Mortise • Ankle 15-25 degrees internal rotation • Evaluate articular surface between talar dome and mortise • Lateral • Identifies fractures of anterior/posterior tibial margins, talar neck, displacement of talus
Identifies fractures of malleoli distal tibia/fibula plafond talar dome body and lateral process of talus calcaneous AP x-ray:
Tib/fib clear space Tib/fib overlap
Now apply what you’ve learned … • Lateral malleolar fracture • Tib/fib clear space <5mm • Tib/fib overlap >10 mm • No evidence of syndesmotic injury
Mortise X-Ray • Taken with ankle in 15-25 degrees of internal rotation • Useful in evaluation of articular surface between talar dome and mortise
Mortise x-ray: • Medial clear space • Between lateral border of medial malleous and medial talus • <4mm is normal • >4mm suggests lateral shift of talus
Mortise x-ray: • Talar tilt • Normal = -1.5 to +1.5 degrees (ie. Parallel) • Can go up to 5 degrees in stress views • <2mm difference between medial and lateral talar/plafond distances
Lateral x-ray: • Identifies fractures of • Anterior/posterior tibial margins • Talus • Displacement of talus • Os trigonum
Stable vs Unstable • The ankle is a ring • Tibial plafond • Medial malleolus • Deltoid ligaments • calcaneous • Lateral collateral ligaments • Lateral malleolus • Syndesmosis • Fracture of single part usually stable • Fracture > 1 part = unstable Source: Rosen
Walking the walk …. Talking the talk Ortho is on the phone. They ask you to describe the fracture….
Lauge-Hansen: • 15 basic types of injury in 5 major categories • Described by two words • Position of foot at time of injury • Direction of talus within mortise causing fracture • Eg: supination-external rotation • Further subdivided into worsening areas of injury • Impossible to remember and clinically useless in the ED
Danis-Weber • Defines injury based on level of fibular fracture • A=below tibiotalar joint • No disruption of syndesmosis • Usually stable • B=at level of tibiotalar joint • Partial disruption of syndesmosis • C=above tibiotalar joint • Disrupts syndesmosis to level of fracture • unstable • THE MORE PROXIMAL THE FIBULAR # THE MORE SEVERE THE INJURY
AO classification: • Similar to Danis-Weber scheme • Takes into account damage to other structures (usually medial malleolous) • ~2 pages of classifications • Remember them all for your exam!
Pott’s classification: • Easy to remember • First degree • unimalleolar • Second degree • bimalleolar • Third degree • trimalleolar
Lateral Malleolar FractureDanis-Weber A • Mechanism • Suppination/adduction (inversion) • Mortise intact • Stable fracture • Treatment • Below knee cast
Bimalleolar (lat & post malleoli) • Mechanism • Inversion • Avulsion of posterior malleolus (post tibiofibular ligament) • Medial mortise wide • Suggests instability • Management • Posterior slab • Orthopedic consult Source: McRae’s Practical Fracture Treatment
Trimalleolar Fractures • Unstable • Multiple ligamentous injuries • Usually involves syndesmosis • Treatment • Posterior slab • Urgent orthopedic consultation • ORIF
CASE 5 Source:Rosen
Pilon (tibial plafond) fractures • Fracture of distal tibial metaphysis • Often comminuted • Often significant other injuries • Mechanism • Axial load • Position of foot determines injury • Treatment • Unstable • X-ray tib/fib & ankle • Orthopedic consultation Source:Rosen
Tillaux Fracture • Occurs in 12-14 year olds • 18 month period when epiphysis is closing • Salter-Harris 3 injury • Runs through anterolateral physis until reaches fused part, then extends inferiorly through epiphysis into joint • Visible if x-ray parallel to plane of fracture (may require oblique) • Mechanism • External rotation • Strenth of tibiofibular ligament > unfused epiphysis
Tillaux Fracture • Management • Inadequate reduction of articular surface can lead to early OA • Gap >2mm in articular surface is unacceptable • Advanced imaging techniques may be necessary • Early orthopedic consultation • Non-displaced • NWB below knee cast • Displaced • surgery
Case 7 Source: Rosen
Maisonneuve Fracture • Mechanism • Eversion + lateral rotation • May cause medial malleolar fracture or deltoid ligament disruption • Injury proceeds along syndesmosis and involves proximal fibula • Always rule out Maisonneuve fracture in medial malleolar/ligamentous injury
Maisonneuve Fracture • Mechanism • Eversion + lateral rotation • Causes medial malleolar fracture or deltoid ligament disruption
If injury proceeds along syndesmosis it involves proximal fibula = Maisonneuve Fracture • Always rule out Maisonneuve fracture in medial malleolar/ligamentous injury
As talus continues to rotate • Posterior tib-fib ligament ruptures • Interosseous membrane rips • Gross diastasis • Dupuytren fracture – dislocation of the ankle