Download
1 / 45
450 likes | 571 Views
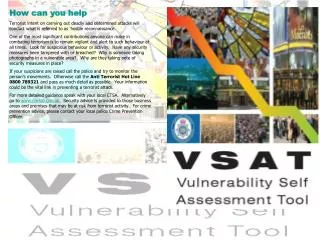
How can molecular imaging help the radiation oncologist. Stephen M. Hahn Department of Radiation Oncology University of Pennsylvania School of Medicine SNM Winter Meeting February 7, 2009.

E N D
How can molecular imaging help the radiation oncologist Stephen M. Hahn Department of Radiation Oncology University of Pennsylvania School of Medicine SNM Winter Meeting February 7, 2009
Disclosures:Research Funding for 18F-EF5 from Varian, Inc.EF5 & 18F-EF5 are investigational diagnostic agentsOther experimental investigational PET agents will be discussed
Outline • Why is Nuclear Medicine important to Radiation Oncology? • What is IGRT & what is the role of Nuclear Medicine? • How does IGRT relate to the biology of human cancers? • The future of IGRT & Nuclear Medicine
Why Is Nuclear Medicine Important to Radiation Oncology? • Ours is a technology-laden field with hardware and software advances moving at a rapid pace often occurring more quickly than we can rationally incorporate them into clinical practice. • We are treating smaller target volumes with tighter margins • The margin for error is smaller. This requires image guidance & provides the rationale for IGRT
Therapeutic Gain • Therapeutic Index is a measure of the relative effect of treatment on the tumor compared to normal tissues • The goal of delivering radiation therapy is always to maximize the effect on tumor and minimize the effect on normal tissues-improving the therapeutic index
Tumour control Effect of underdosage and overdosage Late normal tissue damage Effect Tumor Dose
The irradiated volumes ICRU 62 report • GTV = Gross Tumor Volume • = Macroscopic tumor • CTV = Clinical Target Volume • = Microscopic tumor • PTV = Planning target Volume • = IM + SM PTV
IGRTImage Guided Radiation Therapy • Image guidance in radiation therapy is currently in vogue because of the increasingly conformal nature of radiation delivery to tumors • Our challenge is to prove that IGRT improves patient outcome • However, the importance of image guidance lies in the ability to bridge the gap between the physical characteristics of radiation therapy and cancer biology
Definition of IGRT • Image-guided Treatment Planning • Tumor localization FDG-PET • Incorporation of biological factors – hypoxia, signaling pathways, normal tissue function • Image-guided Delivery of Radiation • Systematic errors • Random errors • Image-guided Response Assessment • Image-guided Dose Assessment • Proton therapy – on board PET imaging
Why is IGRT Important? • Physical targeting becomes particularly important in appropriate clinical situations where methods of dose delivery are being used with tight margins around planning volumes • through more precise delineation of tumor vs. normal tissue • through more precise localization of the target volume in the treatment room • through accurate assessment of dose delivery to tumor & normal tissues
Image Guided Treatment Planning • The use of imaging to distinguish tumor from normal tissues which permits the delineation of the appropriate target volume (PTV). • CT Simulation • MRI Simulation • PET-CT fusion • 4D CT – account for organ motion • Functional imaging – tumor physiology
Vander wel et al. Int J Radiat Oncol Biol Phys. 2005 Mar 1;61(3):649-55. Influence of imaging on the irradiated volume: e.g. CT-PET simulator
MUNICON II Trial • Neoadjvant chemotherapy has become an accepted therapy option for patients with esophageal cancer • Early response assessment would allow for identification of patients who should immediately receive surgery • Hypothesis: FDG-PET accurately identifies those patients with non-responding tumors • Lordick et al. Lancet Oncol 2007
MUNICON II Trial • 119 pts with locally advanced esophageal cancer receiving neoadjuvant chemotherapy • Prospective evaluation • Hypothesis driven • Metabolic Responders defined as those patients with 35% or greater decrease in SUVs • Lordick et al. Lancet Oncol 2007
MUNICON II Trial • Metabolic responders-additional chemo • Non-responders-immediate surgery • Primary endpoint – median overall survival of responders and non-responders • 110 evaluable for response assessment • 54 responders • Median follow up 2-3 years • Lordick et al. Lancet Oncol 2007
Study Design – Lordick et al. Lancet Oncol Volume 8, Issue 9, September 2007, Pages 797-805
Transaxial positron emission tomography images of two patients at baseline and day 14 Ott, K. et al. J Clin Oncol; 24:4692-4698 2006
MUNICON II Trial • Median survival • Responders-not reached • Non-responders-25.8 months • Major histological responses (<10% tumor) • 58% responders • 0% non-responders • Lordick et al. Lancet Oncol 2007
Event-free survival and overall survival in 110 patients assessed with PET for early metabolic response to neoadjuvant chemotherapy Lordick et al. Lancet Oncol Volume 8, Issue 9, September 2007, Pages 797-805
Event-free survival and overall survival according to metabolic and histopathological responses in 104 patients that underwent surgery Lordick et al. Lancet Oncol Volume 8, Issue 9, September 2007, Pages 797-805
MUNICON II Trial • Median survival • Responders-not reached • Non-responders-25.8 months • Major histological responses (<10% tumor) • 58% responders • 0% non-responders • Lordick et al. Lancet Oncol 2007
Event-free survival and overall survival according to metabolic and histopathological responses in patients who had surgery Lordick et al. Lancet Oncol Volume 8, Issue 9, September 2007, Pages 797-805
Biological Targeting • Can we define common signal transduction pathways that regulate/alter the radiation sensitivity of solid tumors? • Can agents that target these pathways be taken into the clinic to alter outcome?
Intrinsic radioresistance is promoted by PI3Kinase activation receptor activation? RAS PI3K PTEN PDKs RAC P70S6K AKT RHO
Dissecting the signalling pathways that affect radiation survival MAPK Cetuximab Gefitinib EGFR L744,832 Genetic knockout siRNA RAS LY294002 Add-back siRNA PI-103 BAY439006 PI3K RAF Rac MEKK4 siRNA AKT VIII PD98059 U0158 JNK MEK P38 MAPK MTOR AKT SB203580 Rapamycin p70S6K
Inhibition of EGFR & Radiation • Preclinical studies demonstrate that inhibition of EGFR in combination with radiation leads to radiosensitization • A recently completed Phase III trial of C-225 & radiation in HNC showed improved survival, locoregional control, & mild increase in skin reactions compared to radiation alone • This study is important because it supports the principle of using targeted therapy to improve the therapeutic index of radiation • Bonner JA et al. NEJM 2006
The use of HIV protease inhibitors as radiosensitizers • Insulin resistance and diabetes are recognized side effects of HIV protease inhibitors (HPIs) and may reflect inhibition of Akt signaling • Hypothesis: HPIs will selectively radiosensitize human tumors that have activation of the PI3K-Akt pathway
NLF is an in vitro and in vivo radiosensitizer - + P-Ser 473 Akt Total Akt Gupta, AK et al Cancer Res 65:8526, 2005
EF5 Hoechst Merged NLF Control Pore N et al. Cancer Res 2006 EF5 Binding control NLF-treated
Biological Targeting in Radiation Therapy • The ras-PI3K-Akt pathway appears to be important in radiation response. Components of this pathway are reasonable targets for clinical trials • One mechanism of radiosensitization is altering the tumor microenvironment which may provide a useful imaging tool for monitoring the biological effect of targeted agents in clinical trials • Nuclear Medicine (PET) techniques are likely to be the most useful for evaluating novel imaging targets
Hypoxia Imaging with EF5 • Evans & Koch have developed & tested a biopsy-based test to identify the presence and level of hypoxia in tumors: EF5 • Studies in humans have shown that hypoxia is associated with radiation resistance, metastasis, and poor clinical outcome • EF5 Binding, Analyzed as a Continuous Variable Predicts Time to Tumor Recurrence (p= 0.003) Evans et al. CCR 2005 • In the small group of patients studied, hypoxia, as measured by EF5 increases with the biologic aggressiveness. Prognostic factor for grade 3 & 4 tumors? Evans, SM et al. Clin Cancer Res 2005
Conversion of EF5 binding to pO2 10 1 (%) 0.1 pO2 % BINDING LABEL 10.0 % 1.0 Physiological 2.5% 3.0 Modest Hypoxia 0.5% 10.0 Moderate Hypoxia 0.1% 30.0 Severe Hypoxia Oxygen Partial Pressure 0.01 1.0E-03 1.0E-07 1.0E-06 1.0E-05 1.0E-04 * EF5 Binding (pmol/cell/hr)
18-F EF5 PET Images of de novo GBM MRI Post-GAD MR-PET Fusion 18F-EF5 PET Evans,Koch 2006
Post-GAD 3 hr F18 EF5
Hypoxia PET Imaging • Hypoxia affects radiation response and appears to be associated with signaling pathway changes in tumors that are associated with radiation resistance • Can we use hypoxia PET imaging in the treatment planning and delivery process to increase dose to radiation “resistant” regions? • Can we use hypoxia PET imaging as a surrogate for signaling pathway activation and therefore guide therapies? • Can we use hypoxia PET imaging to assess response to these agents?
Take Home Messages • Image-guidance especially the use of FDG-PET has become crucial in the era of conformal radiotherapy • Treatment planning – target delineation • Incorporation of biological parameters in treatment plans • Assessment of response • FDG-PET imaging important for target delineation in several tumors • In the future • Identification of hypoxia and other extrinsic causes of radiation resistance • Exploitation of biological data from imaging studies to individualize therapy • Assessment of proton dose in real time with use of on-board PET imaging
Many questions need to be answered • What acquisition & processing protocols should be used to optimize the XRT treatment planning process? • What threshold for SUVmax should be used to define the GTV? • How do we identify and address tumor heterogeneity? • How does PET imaging help with the problem of tumor/organ motion? • How do we incorporate important radiobiological parameters into the treatment equation? • Tumor microenvironment/hypoxia • Signaling pathways • Tumor cell repopulation • Predictors of normal tissue toxicity
Amit Maity Nabendu Pore Zibin Jiang Shuang Liu Don Solomon Chaitanya Divgi Joel Karp Sydney Evans Cam Koch Eric Bernhard Anjali Gupta George Cerniglia Gary Kao W. Gillies McKenna Acknowledgements