Download
1 / 61
670 likes | 1.16k Views
Aminoglycosides & Spectinomycin. Part A Aminoglycosides. Overview. History and Source : the research made by Waksman and coworks within 1939-1943 Clinical Applications: for the treatment of aerobic G - bacterial infections and tuberculosis

E N D
Overview • History and Source : the research made by Waksman and coworks within 1939-1943 • Clinical Applications: for the treatment of aerobic G- bacterial infections and tuberculosis • Two classes: crude product and semisynthetic derivative
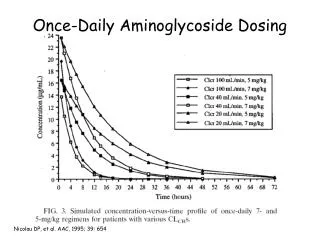
Peak Concentration Blood Concentration Bacterial growth is inhibited long after concentration below the MIC MIC Time (h) General properties 1. Antimicrobial activity: i) rapidly bactericidal to resting bacterium ii) broad-spectrum: G- bacilli and cocci,G+ organisms,TB iii) more active at alkaline iv) concentration-dependent activity v) the duration of post antibiotic effect (PAE) is concentration- dependent (10 hours). vi) first exposure effect (FEE)
General properties 2. Mechanism of action: • inhibit protein synthesis • act as Ionic-absorbent, act directly on permeability of the cell membrane of bacterium.
P A Inhibiting protein synthesis: Aminoglycosides
2.Mechanism of action -inhibit protein synthesis i) Interfering with the initiation complex of peptide formation. ii) Inducing misreading of mRNA, which causes the incorporation of incorrect amino acid into peptide, resulting nonfunctional or toxic protein. iii) causing breakup of polysomes into nonfunctional monosomes. iv) disrupt the normal cycle of ribosomal, make the ribosomal exhausted.
3. Mechanism of resistance produces enzymes Changes of Porins Altered ribosomal subunit
Mechanism of Resistance i) The microorganism produces a transferase enzyme or enzymes that inactivate the aminoglycoside by adenylyation, acetylation, or phosphorylation. ii) Impaired entry of aminoglycoside into the cell. iii) The receptor protein on the 30S ribosomal subunit may be deleted or altered as a result of mutation.
General properties ADME i) Absorption: not absorbed after po, but rapidly absorbed after IM. ii) Distribution: Binding to plasma protein is minimal, do not enter cell, nor do they cross BBB,but they cross the placenta, reach high concentrations in secretions and body fluids. Tissue level is low expect in the cortex of kidney. iii) Elimination: excreted mainly by glomerular filtration. If renal function is impaired, accumulation occurs with a increase in those toxic effects which are dose related.
General properties Clinical Uses • be mostly used against aerobicG-bacteria (bacilli, enteric) and in sepsis, be almost always used in combination with b-lactam antibiotic and fluoroqunolones • Tuberculosis
General properties Adverse reactions i) Ototoxicity • involves progressive damage to and destruction of the sensory cells in the cochlea and vestibular organ in the ear (irreversible!! Auditory and vestibular damage). ii) Nephrotoxicity • consists of damage to the kidney tubules and be reversed if stop using.
General properties Adverse reactions iii) Neuromuscular blockade (paralysis) • generally occurred after intra-pleural or intra-peritoneal instillation of large doses of an aminoglycosides • Calcium salt or inhibitor of cholinesterase (neostigmine) is the preferred treatment for this toxicity. iv) Allergic reaction • skin rashes fever, eosinophiliay ,anaphylactic shock, etc.
Aminoglycosides • Streptomycin • Gentamicin • Tobramycin • Amikacin • Netilmicin • Neomycin • Kanamycin • Arbekacin • Dibekacin • Micronomicin • Sisomicin • Etilmicin • Isepamicin • Astromicin
Streptomycin 1. ADME i) Absorption:IM ii) Distribution: mainly at extracellular fluid, crosses the BBB and achieves therapeutic concentrations with inflamed meninges. iii) Excretion:90%, kidney 2.Clinical uses i) plague and tularemia: combination with an oral tetracycline. ii) tuberculosis: as first-line agent iii) bacterial endocarditis: (enterococcal, viridans streptococcal, etc.), streptomycin and penicillin produce a synergistic bactericidal. 3. Adverse reactions i) Allergic reaction skin rashes, fever, anaphylactic shock ii) Ototoxicity: disturbance of vestibular function, deafness of newborn iii) Nephrotoxicity iv) Neuromuscular blockade (paralysis):Myasthenia Gravis, anesthetics, scoline
Gentamicin 1. ADME Gentamicin can accumulate in cortex of the kidney . 2.Clinical use : i) serious G- bacillary infections (sepsis, pneumonia, etc.). ii) infection induced by enterococcal, viridans streptococcal, staphylococcal etc. (in combinationwith other antibiotics, e.g. b-lactams) iii) prevent the infection induced by operation (e.g., gastrointestinal operation ) iv) local application or intrathecal administration (rarely use) 3. Adverse reactions i) Nephrotoxicity (reversible and mild) ii) Ototoxicity (irreversible!) iii) Nausea and vomiting etc.
Tobramycin 1.antimicrobial activity & pharmacokinetics: very similar to those of gentamicin; has cross-resistance to gentamicin. 2. Adverse reactions: Ototoxicity and Nephrotoxicity (may be less than dose gentamicin).
Netilmicin 1. similar to gentamicin & tobramycin in its pharmacokinetic properties. 2. broad spectrum, against aerobic G- bacilli. 3. tolerance to many aminoglycosides (gentamicin, tobramycin) - inactivating enzymes. 4. less toxic
Amikacin 1.Antibacterial activity: the broadest in the group. 2.Clinical uses : • Treatment of G-bacillary infections which resistance to gentamicin and tobramycin. • Most strains resistance to amikacin found is also resistance to other aminoglycosides. • combination with b-lactams, produce a synergistic bactericidal. 3. Adverse reactions i) Ototoxicity ii) Nephrotoxicity iii) Neuromuscular blockade (paralysis) iv) skin rashes, fever, nausea and vomiting etc.
Representative drugs Erythromycin Dirithromycin Meleumycin Josamycin Acetylspiramycin Midecamycin Penicillin-resistant Staphylococcus Penicillin-allergic patients First generation Rokitamycin Roxithromycin Clarithromycin Azithromycin Acetylmidecamycin flurithromycin Second generation Penicillin-resistant Staphylococcus Penicillin-allergic patients
Antibacterial spectrum • board bactericidal or bacteriostatic drugs • G+ and G- bacteria, cocci, Neisseria gonorrhea, gram-positive bacilli, and spirochetes, mycoplasma,rickettsiosis • 2. Mechanisms • Inhibition of protein synthesis • (1) reversible binding to 50S subunit of • ribosome (23S rRNA) • (2) L22 protein binding in 50S subunit, • lead to disruption of ribosome
3. Clinical Usage (1) Streptococci infection (2) Legionella pneumophila (3) infection from spirochetes, mycoplasma,rickettsiosis 4. Adverse reaction (1) GI (2) hepatic damage (3) superinfection: infection that occurs while treating another infection. e.g. oral fungal infection (4) Ototoxicity (5) allergic reaction
Lincomycin & Clindamycin • Antibacterial spectrum • (1) board bactericidal or bacteriostatic drugs, similar to the macrolides • (2) Anaerobic G+ and G- bacteria • 2. Mechanisms • Inhibition of protein synthesis • L16 protein binding in 50S subunit, • lead to disruption of ribosome. Avoid to using with erythromycin • (same binding sites), antagonistic effects.
3. Clinical Usage (1) Aerobic bacteria (2) anaerobic bactreria (3) infection from staphylcoccus in bone tissues (osteomyelitis ) 4. Adverse reaction (1) GI (2) hepatic damage (3) allergic reaction
Chlortetracycline Oxytetracycline tetracycline Natural products Doxycycline Methacycline minocycline Semisynthesis
Antibacterial spectrum • board bacteriostatic drugs • G+ and G- bacteria, cocci, spirochetes, mycoplasma,rickettsiosis, • chlamydia. • 2. Mechanisms • (1) Cell membrane transportation • (2) Inhibition of protein synthesis • 30S subunit of ribosome • (3) permeability
3. Clinical Usage (1) spirochetes (2) mycoplasma (3) rickettsiosis, (4) chlamydia (5) bacteria 4. Adverse reaction (1) GI (2) hepatic damage (3) superinfection: infection that occurs while treating another infection. e.g. oral fungal infection (4) teeth and bone (5) renal toxicity (6) photosensitized reaction (7) ototoxicity
Antibacterial spectrum • board bacteriostatic bactericidal drugs • G+ and G- bacteria, spirochetes, mycoplasma,rickettsiosis, • 2. Mechanisms • Inhibition of protein synthesis • 70S ribosome complex, 50S • hematopoietic stromal cellin bone marrow, • mammary70S is similar to baterial 70S, lead to bone marrow suppression
3. Clinical Usage (1) bacterial meningitis, purulent Meningitis in Children (2) Corynebacterium diphtheriae infection (3) eye infection (bacteria) (4) anaerobic infection 4. Adverse reaction (1) GI (2) Gray baby syndrome: disturb the ribosome function in mitochondria ability of detoxication via glucuronic acidconjugation ability of renal excretion (3) bone marrow suppresion: AA, anemia, granulocytopenia, thrombopenia
Vancomycins • Antibacterial Mechanism • Inhibiting cell wall synthesis by binding to the D-Ala-D-Ala terminus of nascent peptidoglycan penta-peptide. • Resistance • occurred because of the alteration of D-Ala-D-Ala to the D-Ala-D-Ser.
Vancomycins • ADME • Oral administration (poorly absorbed). • Intravenous administration, is excreted by glomerular filtration (accumulates when renal function is impaired). • Widely distributed in the body, including CSF when the meninges is inflamed.
Vancomycins • Clinical Uses • 1) severe infection caused by MRSA etc. • 2) alternative for b-lactam • 3) enterococcal or staphyococcal endocarditis (combination with gentamicin). • 4) pseudomembranous colitis • ***Overuse should be avoided, in view of limited options for treatment of resistant gram positive infections.
Vancomycins • Adverse Reactions • 1) Hypersensitive reaction • (e.g. red man syndrome) • 2) Ototoxicity • 3) Nephrotoxicity • 4) Gl effects, Phlebitis etc.
Part B Synthetic antimicrobial agents
Generation Example time 1 Nalidixic acid 1962 2 Pipemidic acid 1973 3 Norfloxacin1980’s 4 Clinfloxacin 1990’s Synthetic antimicrobial agents • Quinolones • Sulfonamides • Other Synthetic antimicrobial • Trimethoprim, Nitrofurans
5 4 R 6 3 8 1 2 R 7 R First generation fluoroquinolones
General properties of Quinolones Antimicrobial activity & spectrum: (1) bactericidal and have significant PAE. (2) aerobic G- bacteria, Pesudomonas, aerobic G+bacteria, Chlamydia spp., Legionella pneumophila , anaerobic bacteria, mycobacteria, multiple-resistance strains.
DNA gyrase Topoisomerase Mechanism of action Key enzymes in DNA replication: bacterial DNA is supercoiled.
porin DNA gyrase Topo isomerase Gram (-) Gram (+) Mechanism of action
DNA gyrase Catalytic subunite Fluoroquinolones: 4 stacked molecules DNA gyrase ATP binding subunite Mechanism of action
decreased permeability active efflux system porin DNA gyrase Topo isomerase mutation of the enzymes Gram (-) Gram (+) Mechanism of resistance
ADME of fluoroquinolones • Absorption: well absorbed; bound by divalent cations • Do not administer with iron, magnesium, calcium • Distribution: all distribute widely (even in CSF), and most concentrate in urine • Metabolism: • hepatic metabolism diminishes the activity of norfloxacin and ciprofloxacin • Several have predominately hepatic clearance (Grepafloxacin, Sparfloxacin, Trovafloxacin) • Excretion: urinary excretion predominates for the first generation fluoroquinolones