Download
1 / 35
350 likes | 537 Views
Survival Analysis and the ACT study. Laura Gibbons, PhD Thanks to An Introduction to Survival Analysis Using Stata. Acknowledgement. Funded in part by Grant R13 AG030995 from the National Institute on Aging

E N D
Survival Analysis and the ACT study Laura Gibbons, PhD Thanks to An Introduction to Survival Analysis Using Stata
Acknowledgement • Funded in part by Grant R13 AG030995 from the National Institute on Aging • The views expressed in written conference materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department of Health and Human Services; nor does mention by trade names, commercial practices, or organizations imply endorsement by the U.S. Government.
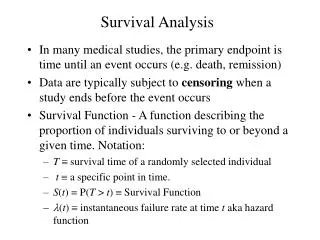
What is survival analysis? • Time to event data. • It’s not just a question of who gets demented, but when. • Event, survive, and fall are generic terms.
ACT example Risk for Late-life Re-injury, Dementia, and Death Among Individuals with Traumatic Brain Injury: A population-based study Kristen Dams-O’Connor, Laura E Gibbons, James D Bowen, Susan M McCurry, Eric B Larson, Paul K Crane. J NeurolNeurosurg Psychiatry 2013 Feb;84(2):177-82.
TBI-LOC = Traumatic Brain Injury with Loss of Consciousness Outcomes (different ways of defining failure) • TBI-LOC during follow-up • Dementia • Death
Survival function • The number who survive out of the total number at risk • In this example, “failure” is a TBI-LOC after baseline. • 4225 participants, with 96 TBI-LOC after baseline.
Hazard function • The probability of failing given survival until this time (currently at risk) • The hazard function reflects the hazard at each time point. • It’s usually easier to look at the cumulative hazard graph.
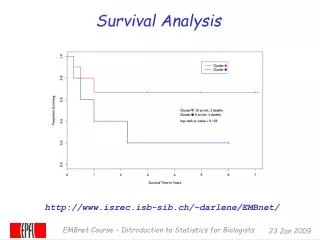
Cumulative Hazard for TBI with LOC (with 95% confidence bands)
Think carefully about onset of time at risk • Study entry • Time-dependent covariates • What to do about exposures which occur before study entry (left truncation)
ACT : TBI-LOC during follow-up • Used study entry as onset of time at risk • Exposure: report of first TBI-LOC at baseline None (n = 3619) At age<25 (n=371) At age 25-54 (n=104) At age 55 to baseline (n=131) • No time-dependent covariates for this example
Time axis Continuous – exact failure time is known Discrete – time interval for failure is known
ACT onsetdate for dementia outcomes The midpoint between the two study visits (biennial and/or annual) that precede the date of the consensus of dementia. The date of the consensus of dementia is defined as the earliest consensus that resulted in a positive diagnosis of dementia (DSMIV) and that was not later reversed as a false positive.
Age as the time axis • Makes sense in an aging study. • Often modeled as baseline age + time. Ties • Multiple events occurring at the same time. • Make sure your software is handling this the way you want.
Think carefully about censoring • Censoring: The event time is unknown • No longer at risk • Missing data – random or informative? • Hope it’s noninformative [Distribution of censoring times is independent of event times, conditional on covariates. ~ MAR.]
Right censoring Event is unobserved due to • Drop out • Study end • Competing event (more on this later) Interval censoring • Know it occurs between visits, but not when • Assume failure time is uniformly distributed in that interval • An issue in ACT (hence onsetdate)
Left censoring The event occurred before the study began. • What about those whose TBI-LOC resulted in death or dementia before age 65? They are not in our study. • Worry about this one. Left truncation Onset of risk was before study entry. • We used our 4-category exposure, but risk really must be defined as “TBI-LOC before age 25 and not left-censored”, etc.
ACT censoring variables • Competing event: onsetdate (dementia) or • Visit date (visitdt) • Withdrawal date (withdrawdt) (The FH data does not include anyone who withdrew.) • Death date (deathdt)
Modeling Non parametric – Kaplan-Meier
Log-rank test for equality of survivor functions | Events Events p | observed expected ---------------------------+------------------------- No TBI-LOC before baseline | 66 82.70 TBI-LOC before baseline | 30 13.30 ---------------------------+------------------------- Total | 96 96.00 chi2(1) = 24.44 Pr>chi2 = 0.0000
Semi-parametric (Cox) Assumes the hazards are proportional • Looks like a reasonable assumption here, but we looked at a variety of graphs and statistics to make sure.
Hazard Ratios Baseline report of age at first TBI with LOC as a predictor of TBI with LOC after study enrolment, controlling for age, sex, and years of education. Age at first TBI Late life TBI with LOCwith LOC cases/person years HR (95% CI) None prior to baseline 66/21,945 1 (Reference) < 25 15/2147 2.54 (1.42, 4.52) 25-54 6/678 3.24 (1.40, 7.52) 55-baseline 9/798 3.79 (1.89, 7.62)
Model checking • Proportional hazards assumption • Covariate form • Baseline, lag or current visit covariate • Et cetera
Parametric Can be proportional hazard models • Exponential. Constant baseline hazard. • Weibull. Hazard is monotone increasing or decreasing, depending on the values for a and b. • Gompertz. Hazard rates increase or decrease exponentially over time. • See Flexible Parametric Survival Analysis Using Stata for many more.
Accelerated failure time • Risk is not constant over time. • Time ratios. Ratios > 1 indicate LONGER survival.
Types of accelerated failure time(AFT) models • Gamma. 3 parameter. Most flexible. Fit a gamma model and see which parameters are relevant. • Exponential, Weibull can also be formulated as AFT models. In the Weibull model, the risk increases over time when β > 1. • Log-normal. The hazard increases and then decreases. • Log-logistic. Very similar to log-normal.
Baseline report of TBI-LOC and the risk of dementia • Proportional hazards assumption not tenable. • The log-logistic AFT model was the winner, reflecting an increased risk over time. • You can compare AICs to pick best model, or pick one based on your hypothesis.
Our AFT model for any dementia • Controlling for baseline age, gender and any APOE-4 alleles • Remember that TR > 1 => longer survival
TBI-LOC is NS. Older baseline age and APOE associated with shorter survival. Female and education associated with longer survival. ------------------------------------------------ _t | TR [95% Conf. Interval] -------------+---------------------------------- base4 | <25 | 1.02 0.87 1.20 25-54 | 1.04 0.78 1.38 55+ | 1.06 0.81 1.39 | 10 years age | 0.53 0.49 0.57 female | 1.15 1.05 1.26 education | 1.02 1.00 1.04 apoe4 | 0.69 0.63 0.76 ------------------------------------------------
Competing risks • Individuals are at-risk for AD, vascular dementia, other dementias • No longer at risk for one type once diagnosed with another (assuming we’re dealing with first diagnosis) • Use cause-specific hazard functions and cumulative incidence functions.
What is going on in competing risks? • Which is it? • One process determines dementia and another says which type • Two separate processes, and one event censors the other. • In our analysis of TBI-LOC predicting AD, we censored at other dementia diagnoses, but we could have modeled multiple dementia outcomes (assuming adequate numbers). • The competing risk model may be more accurate, because the time to AD and the time to other dementia are probably correlated.
Shared frailty, aka unobserved heterogeneity or random-effects • There may be variability in individuals’ underlying (baseline) risk for an event that is not directly measurable. • One way of dealing with patients from different cities, for example. • The assumption is that the effect is random and multiplicative on the hazard function.
Need to distinguish between hazard for individuals and the population average. • Population hazard can fall while the individual hazards rise. • The frailer individuals have failed already, so the overall hazard rate drops. Yet time is passing, so each person’s risk is still rising.
In a shared frailty model, HR estimates are for time 0. • Covariate effects decrease as the frail fail. • Gamma frailty models. Covariate effects completely disappear over time. • Inverse-Gaussian models. Covariate effects decrease but do not disappear over time.
Other issues in survival analysis not covered today include • Events that can occur more than once (heart attacks, for example) • Parallel processes • Unshared frailty