Download
1 / 35
770 likes | 1.93k Views
Macro-TSH and endogeneous antibody interference in immunoassays. Ellen Anckaert, M.D., Ph.D. Laboratorium Hormonologie & Tumormarkers UZ Brussel. Antibody. Ruthenium. Biotin. Antibody. Antigen. Non-competitive immunoassay principle. Sandwich complex.

E N D
Macro-TSH and endogeneous antibody interference in immunoassays Ellen Anckaert, M.D., Ph.D. Laboratorium Hormonologie & Tumormarkers UZ Brussel
Antibody Ruthenium Biotin Antibody Antigen Non-competitive immunoassay principle
Sandwich complex Non-competitive immunoassay principle
Microbeads Non-competitive immunoassay principle
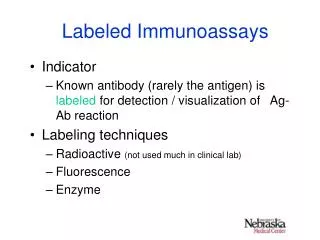
Interference Definition: “interference is the effect of a substance present in the sample that alters the correct value of the result for an analyte (Kroll & Elin, 1994) Immunoassay design determines the sensitivity of the assay to interference
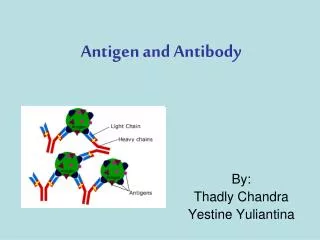
Antibody interference in thyroid hormone assays Antibodies against assay antibodies Heterophilic antibodies Autoantibodies against thyroid hormones Anti-TSH (macro-TSH) Anti-thyroglobulin antibodies Anti-T4, Anti-T3 antibodies Antibodies against assay antibody detection molecules
Interferences due to endogeneous antibodies against assay antibodies • Possible clinical consequences: • Misclassification of monitoring results • Unnecessary follow-up examinations • False therapy decisions • Unfavorable patient prognosis
Mechanisms of interference by heterophilic antibodies Exclusive binding of capture or detector antibody only => Falsely lowered result Bridging of capture and detector antibodies => Falsely elevated result
Assay design: whan can the manufacturer do to reduce heterophilic antibody interference ? No protection Use of blocking proteins Fragmentation of Antibodies Use of chimeric MABs Interference level: High low extremely low
1. Addition of blocking antibodies • Addition of a “blocking agent” of the same species as the assay antibodies: • animal serum • animal immunoglobulin • aggregated mouse monoclonal IgG (MAK33) to eliminate strong HAMA interferences, usually therapy induced
2. Fragmentation of antibodies Use of Fab or F(ab’)2 fragments
3. Chimeric Antibodies Constructed from 2 different species (mouse / human ) Fc-fragment cleaved off Variable region from mouse IgG C1 constant region from human IgG
Heterophilic antibody / HAMA interference Prevalence of interference depends on the immunoassay (IA) method Bjerner 2002 (CEA, 11.261 patient samples) unblocked IA 4% blocked IA (Fc removal) 0.1% blocked IA (Fc removal – MAK33) 0.06% Boscato 1986 (hCG, 668 healthy subject samples) unblocked IA 15% blocked IA 0.6% Ward 1997 (TSH, 21.000 patient samples) blocked IA 0.03% addition of “blocking reagent” reduces interference, but is no garantee for complete elimination of interference estimated prevalence: 0.03 – 3%
What can the lab do to detect immunoassay interference by heterophilic antibodies? A negative interference test does not exclude interference
Macro-TSH • Macro-molecule composed of TSH and anti-TSH immunoglobulin • Reduced renal clearance leads to accumulation of macro-TSH • Reduced biological activity • Patients are clinically euthyroid • Immunoreactivity is variable and reduced compared to native TSH • spuriously elevated TSH levels to a variable degree using different immunoassays • low recovery of added TSH
Case report macro-TSH (1) • 60 year old man, clinically euthyroid • TSH1 232 mIU/l (0.45-5 mIU/l) • FT4 10 pmol/l (10-23 pmol/l) • TPO Ab 496 IU/ml (0-50 IU/ml) • Tg Ab Neg • anti-TSH receptor Abs Neg • Test with an alternative immunoassay method • TSH2 122mIU/l • Test dilution linearity3: • TSH 1:1 122mIU/l • TSH 1:10 165 mIU/l (135% recovery) • Test for antibodies against assay antibodies • RF Negative • Heterophilic blocking tubes No interference detected • 1 Vitros 5600, Ortho Clinical Diagnostics; 2 Advia Centaur, Siemens Healthcare Diagnostics 3 TSH assay diluent and immunoassay: Advia Centaur Loh T P, JCEM 2012
Case report macro-TSH (2) • PEG-precipitation of high molecular weight proteins • Pre-PEG TSH 122mIU/l • Post-PEG TSH 3.9 mIU/l (3.2% recovery) • Presumable interference: • Macro-TSH = macro-molecule formed between TSH and autoimmune anti-TSH Ig • Heterophilic antibodies undetected by HBT • Testing the presence of excess TSH binding capacity = free anti-TSH antibody • sequestration of added TSH (hypothyroid serum) • macro-TSH has reduced immunoreactivity compared to native TSH • RESULT: low recovery (85%) • Thyroid stimulating Ig bioassay: 120% (normal: 50-179%) • Consisitent with clinical euthyroid state • Suggests low biological activity of macro-TSH * Advia Centaur, PEG recovery in ‘normal’ euthyroid patient serum was 40% Loh T P, JCEM 2012
Confirmation of macro-TSH by gel filtration chromatography Patient serum: TSH peak fraction that approximates the molecular size of IgG (dots). Patient serum incubated with hypothyroid serum: immunoreactivity of the HMW fraction, confirming excess TSH binding capacity and macro-TSH (trangles). Loh T P, JCEM 2012
Immunoassays display variable reactivity with macro-TSH TSH measurement by different methods Instrument Manufacturer Reference range TSH (µIU/mL) Elecsys Roche 0.5 5.0 152.0 Centaur Siemens 0.4 4.0 20.5 Lumipulse Fuji Rebio 0.61 4.68 112.4 Architect Abbott 0.35 4.94 9.8 Sakai, Endocr J 2009
Prevalence of macro-TSH 15/495 TSH > 10 mIU/l (3%): low recovery after PEG precipitation
Tg antibody interference in Tg immunoassays • Measurement of Tg in follow-up of DTC: should always be accompanied by anti-Tg measurement using a sensitive anti-Tg immunoassay • What can the lab do: • Confirm by an alternative (competitive) immunoassay method • Exogeneous Tg recovery test • low recovery indicates interference • normal recovery does not exclude interference • Anti-Tg antibody prevalence • 10% general population • 25% in DTC • No Tg method completely free from interference • underestimation in non-competitive assay • false elevation is possible in competitive assay
Tg antibody interference in Tg immunoassays Anti-Tg interference in Tg IMA is a common problem
Interference by endogeneous antibodies in FT4 – FT3 assays Anti-T4 and anti-T3 antibodies • Prevalence depends on the selected population and the method of detection • 20% in autoimmune thyroid disease • 6% in non-thyroidal autoimmune disease • 0-2% in healthy individuals • women > men • Mostly IgG subclass, mostly polyclonal • Most patients also have anti-Tg and/or anti-microsomal antibodies • Impact on immunoassay (interference) depends on • the assay format • titer, affinity and specificity of the antibody
* One step method - Labeled Analog + + T4 * FT4 Conjugated Analog Serum Binding Protein Anti - T4 Antibody Bound to Particle X * Separate and Count +
Interference by anti-ruthenium antibodies in Elecsys FT4 – FT3 assays Anti-Ru antibodies • Mainly in areas with textile industry • Use of Ru in dying process of clothing • Ru in environment, clothing or food chain • Estimated frequency of interference in first generation Elecsys FT3 assay (Roche Diagnostics): 0.2% (Sapin, Clin Chem Lab Med 2007)
Roche claims increased protection against anti-Ru antibodies in next generation IA
Case report 28/8/ 5/2/ 11/9 15/5 Normal values 2013 2013 2012 2012 TSH (mIU/l) 0.552 0.344 0.569 0.515 0.27-4.2 FT3 (ng/l) 3.25.9 7.0 6.2 2.6-4.4 FT4 (ng/l) 12.620.8 21.2 19.5 9.3-17.0 Switch to Elecsys FT3 III and FT4 II
FT4 immunoassays are all binding protein-dependent to some extent Increased TBG in pregnancy Genetic abnormalities in binding proteins, drugs that displace FT4 from binding proteins, NTI Anckaert, Clin Chim Acta 2010
Conclusion • Interference in immunoassays • uncommon • exception: anti-Tg interference in Tg IMA • no method is completely free from interference • often unidentified by the laboratory routine quality assurance check • Immunoassay results that are incongruent with the patient’s clinical presentation should be tested for interference • Clinician should be actively encouraged to contact the laboratory in case of any doubt about a result • In case of confirmed interference patients should be informed about the presence of interfering substances in their serum