Download
1 / 71
760 likes | 840 Views
Learn about Leishmania donovani, its prevalence worldwide, pathogenic species, life cycle stages, morphology, transmission, pathology, clinical features, and diagnosis methods.

E N D
Charles Louis Alphonse Laveran France Institute Pasteur Paris, France 1845 - 1922 The Nobel Prize in Physiology or Medicine 1907 "in recognition of his work on the role played by protozoa in causing diseases"
Leishmaniasis is prevalent world wide: ranging from south east Asia, Indo-Pakistan, Mediterranean, north and central Africa, and south and central America.
Species Pathogenic in Humans Leishmania donovani (Laveran 1903) (VL) Leishmania tropica (CL) Leishmania major (CL) Leishmania aethiopica (CL) Leishmania mexicana (CL) Leishmania brazilliensis (MCL)
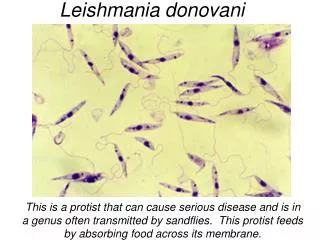
Promastigote Insect Motile Midgut Amastigote Mammalian stage Non-motile Intracellular Morphology Digenetic Life Cycle
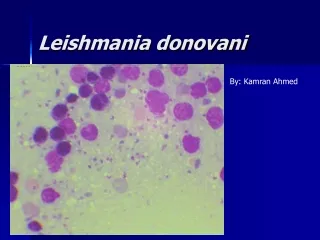
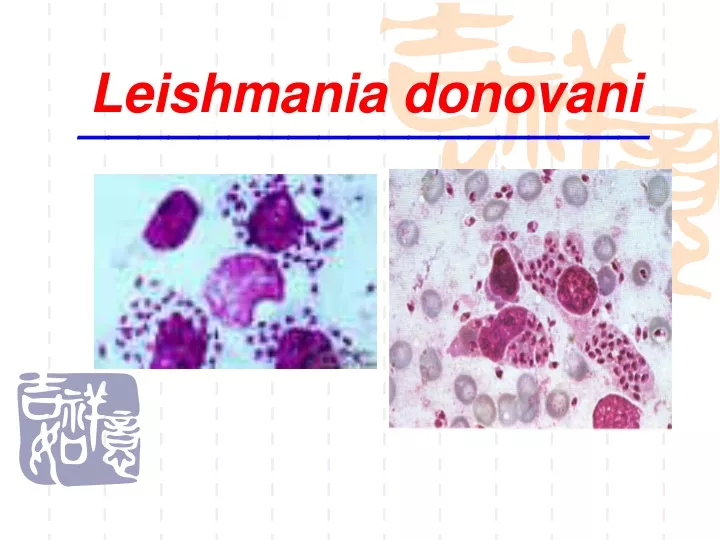
Morphology • Amastigote (leishman-donovan body): • Human phase, reside in macrophage • Very, very minute elliptical body • No free flagellum • Nucleus: deep red, located at one side • Cytoplasm: blue (after right stain) • Kinetoplast; basal body; rhizoplast
Promastigote • elongate form • - 15 - 30 µm long • one nucleus, red stained, central in position, • one anterior flagellum which is just as long as its body length. • a rod-like kinetoplast • a dot-like basal body anterior Flagellum Basal body Kinetoplast Nucleus posterior • Insect • Motile • Midgut
Promastigote: • Vector phase • Reside in the gut of sandfly • Spindle shaped with 1 free flagellum • Nucleus; cytoplasm; kinetoplast; basal body; rhizoplast • Chrysanthemum-like in culture medium
Amastigote • M broken with the release of amastigote which may invade other M, start asexual multiplication again
Promastigote • Fusiform-shaped with 1 free flagellum • Usually gather together in the medium as a mum
Phlebotomus,sandfly • Small,about 1/3 of a mosquito, 3mm, yellow-gray
Life Cycle of Leishmania spp. _________________________________________________________
Life Cycle Promastigote Amasitgote Transformation
Main points of the Life Cycle • 2-host pattern, mammal insect vector (sandfly) • Asexual multiplication occurred either in macrophages or in insect , No sexual development in the host • infective stage: promastigote • mode of infection: biten by sandfly • site of habitation: macrophages • pathogenic stage: amastigotes • diagnostic stage: amastigotes • reservoir host: dogs and rodents
Leishmania donovani PATHOLOGY: Amastigotes multiply in macrophage, destroyed the macrophage eventually rupturing the cell • Free amastigotes then invade the circulatory system.
Parasite Spread Macrophage lysis & parasite release 1. Lymphatic spread 2. Blood spread Target organs the mononuclear macrophagocyte system of the spleen, liver, bone marrow and lymph nodes
Clinical features • Lack of acquired immunity but may gain sterilizing immunity after effectively cured. • Most severe form of the disease, may be fatal if left untreated, Reason: lack of immunity after infection. • Irregular fever for long period is due to the broken piece from parasitized tissue. • Massive hypertrophy of spleen , liver and lymph nodes are caused by the proliferation of mononuclear macrophagocytosis system. Destruction, hyperfunction
Clinical features • Because bone marrow is involved and spleen is hyperfunction, caused anemia. • The number of red blood cells( RBCs), white blood cells (WBC) and platelet all decrease. • Bleeding results from the decrease in blood platelets. • The decrease of liver function and the proliferation of plasma cells bring about the ratio of albumin to globulin is inverted. • Skin lesions – granulomatous response: painless nodules in which amastigote may be found – sometimes self-cured • Nephrosis: IC deposition –type III hypersensitivity. • Emaciation with ascites, darkened skin, fever, bleeding of the gums, immunity decrease. Die of infective complications( noma, Pneumonia).
Visceral Fatal (90% untreated) Liver Spleen Bone marrow Cutaneous Generally Self- healing Skin Mucous membranes Clinical Disease
Profile view of a teenage boy suffering from visceral leishmaniasis. • The boy exhibits splenomegaly, distended abdomen and severe muscle wasting.
Two children with visceral leishmaniasis Splenomegaly
Enlarged spleen and liver in an autopsy of an infant dying of visceral leishmaniasis.
Special clinical features for Kala-azar cases • Post-kala-azar dermal leishmaniasis (PKDL):
Diagnosis • Etiological examination • Puncture smear: bone marrow – safe, first choice • Skin biopsy • Tissue or aspirate cultivation • Animal inoculation
Immuno-diagnosis • Antibody detection • Circulation antigen detection • Molecular biology methods • DNA probe test • PCR
Treatment • Injection of Antimony Gluconate cure rate would be 97.4% • Good nursing • Pentamidine or stilbamidine for antimony-resistant patients • Antibiotics • Spleen excision
Epidemic Links • Source of infection: patients and dogs • Route of infection: sandfly. • Susceptible population: all human beings ( but potent immunity developed after cure)
Prevention • Treat the patients • Suppress the reservoir: dogs, rats, other small mammals and rodents • Suppress the vector: Sandfly • Prevent sandfly bites: Personal Protective Measures
Trichomonas vaginalis (阴道毛滴虫) • Trichomonas vaginalis, a flagellate, is the most common pathogenic protozoan in the countries. It causes trichomoniasis (毛滴虫病). The infection is transmitted sexually.
Morphology • Pear-like in shape, about 10-30x5-15um in size. • four anterior flagella and One posterior flagellum which attaches to pellicle to form an undulating membrane (波动膜). • One nucleus • the axon project posteriorly out of the body. • The motility is jerky & non-directional.
Life cycle: Simple: Only Trophozoite stage. There is no cyst stage. Binary fission of reproduction.
Inhabitation: • Female – Vagina(阴道) , Urethra(尿道); • Male – Urethra (尿道), Prostate glands. • Cause Trichomonas vaginitis, urethritis or prostatitis, i.e. Trichomoniasis.
Diagnosis • 1. Etiological examination The specimen should be obtained from vaginal discharge, prostatic fluid or urine. Normal direct smear may be used for exam. the trophozoites. The typical robust Trichomonas can be seen because of their characteristic jerky motion moving among the epithelial cells. • 2. PCR & DNA probe
Treatment • Metronidazole is the drug of choice for both female & male. • Sexual partners should be treated at same time.
Epidemiology • Like most sexually transmitted diseases, trichomoniasis is prevalent in the sexually active age group in all climates and racial groups. • New born girls appear to be at special risk of acquiring trichomoniasis from an infected mother during passage through the birth canal.
Although the organism died rapidly when dried , exposed to direct sunlight, person to person transmission may occur where there is a lack of sanitary toilets or bathing facilities and a sharing of contaminated clothing or washcloth.
Control 1. Treat patients & Carriers. 2. Pay attention to personal hygiene. 3. Avoidance of sexual contact with infected partners .
opportunistic protozoa opportunistic protozoacan not infect persons with normal immune mechanisms or can cause mild (or latent) infection with asymptomatic to self-limited symptoms . opportunistic protozoamay cause devastating disease in persons whose immune resistance has been weakened by various causes, such as: