Download
1 / 41
410 likes | 567 Views
Hip and pelvis conditions. An orthopaedic overview. History. Characteristic Hip Pains: Dull ache- OA, degenerative, tendinitis/ bursitis Sharp – Impingement, acute sprain, labrum tear, subluxation/dislocation, fracture Pain frequently noted in groin and medial thigh

E N D
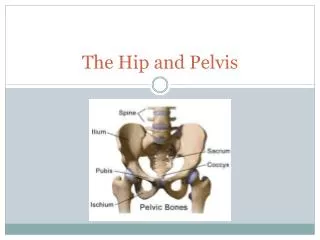
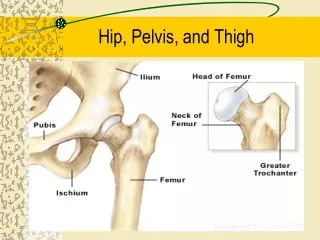
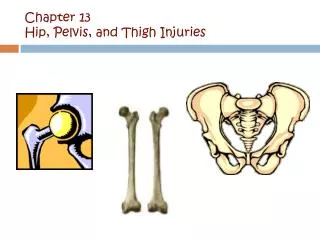
Hip and pelvis conditions An orthopaedic overview
History • Characteristic Hip Pains: • Dull ache- OA, degenerative, tendinitis/ bursitis • Sharp – Impingement, acute sprain, labrum tear, subluxation/dislocation, fracture • Pain frequently noted in groin and medial thigh • Symptoms: pain, weakness, numbness, clicking, giving way • Referred Pain from: Back, Abdomen, Pubic symphysis • Refers Pain to: knee
Pelvic Fracture • Mechanism: High energy: • Motor vehicle crash (50-60%) • Motorcycle crash (10-20%) • Pedestrian versus car (10-20%) • Falls (8-10%) • Crush (3-6%) • Physical examination is specific for pelvic instability, but it has a low sensitivity: high level of suspicion • Pain, swelling, WB/NWB, deformity, crepitus, • Consider Blood loss and signs of shock • GU exam: rectal tone, bladder control, perineum, boggy prostate, scrotal hematoma, hematuria • digital rectal examination has a very low sensitivity for diagnosing pelvic fractures
Pelvic fracture • Management: pelvic binder (T-pod), IV, analgesia, Blood, • Evacuation for surgical assessment • X-ray: pelvic ring- usually disrupted in 2 places • Tile classification: based on the integrity of the posterior sacroiliac complex • Young classification system is based on mechanism of injury • Death most commonly due to hemorrhage or multiple injuries
Acetabular Fracture • Mechanism: high velocity trauma, MVA, falls from height • Multiple fracture patterns: MOI • Pain, non WB, presentations of hip, • Neurovascular exam, abdominal exam, LLD, position of lower limb • Stabilize, IV, analgesic, • Evacuation for X-ray, surgical assessment • 20% concomitant pelvic fracture
Hip fractures: Femoral neck fractures “People come into this world under the brim of the pelvis and leave it by the neck of the femur.”
Femoral Neck Fractures • MOI: Young- MVA, fall from height • Older: simple fall, Osteoporosis: abrupt step, Runners: stress fractures • Acute onset hip pain, unable to WB • O/E: shortened leg, external rotation, painful ROM, crepitus • Neurovascular exam • Stabilize, IV, analgesia • Evacuation for X-ray and surgical assessment
Femoral Neck # • Garden Classification: 1-4 • Treatment: • Young: internal fixation (+/- reduction) • Older: internal fixation non displaced, hemi-arthroplasty
Intertrochanteric Fractures • Extra-capsular fracture including the greater and lesser trochanter (b/w neck and shaft) • Traumatic force to trochanteric area • Acute pain, unable to WB, shortened, ER • Stabilize, IV, analgesic • Evacuation for X-ray, surgical assessment • Treatment: Dynamic Hip Screw fixation
Femoral Shaft Fracture • Mechanism: high energy trauma • Pain, deformity, Non WB • Neurovascular status: urgent reduction? Procedural sedation, blood loss into fracture site…1000mL • Reduction, immobilize, IV, analgesia, Blood products, +/- antibiotics • Evacuation to surgical capability • Surgery: internal fixation- IM nail/ plate
Femoral Shaft # • Complications: • Haemorrhage requiring transfusion • Fat embolism – ARDS • Increased risk of open fracture • Nerve injury • Infection
Distal Femoral Fracture • Supracondylar: above condyles • Condylar, Inter-condylar= intra-articular involvement • Mechanism: high energy force, axial load • Pain, hemarthrosis, non WB, ER, shortened • Immobilize, IV, analgesia • Evacuation for surgical fixation • Complication: femoral artery tear
Which direction is this hip dislocated? • Anterior • Posterior
Femoral Dislocation: Anterior ***Orthopaedic Emergency • Mechanism: blow to knee in hip abduction • Shortened, abducted, ER limb • Neurovascular exam • Stabilize, IV, analgesia, • Urgent Evacuation for X-ray, reduction under sedation/GA • Complications: as per posterior
Hip Dislocation: Posterior ***Orthopaedic Emergency • Mechanism: high force through femur with hip in flexion and adduction (dashboard ) • Pain, Shortened, Add and IR of hip
Hip Dislocation: Posterior • Stabilize, IV, analgesia, • Urgent Evacuation for X-ray- r/o fracture, reduction under sedation/ GA, ORIF • risk of AVN with delayed reduction (>6 hrs)
Osteoarthritis • Slow onset degenerative change often following injury or prolonged exposure to impact, poor biomechanics, congenital hip disorder • Pain into groin and medial thigh • worse with activity, intermittent flares with acute pain and swelling
OA • O/E: trendelenberg gait, decreased ROM, strength deficit, ligament laxity • X-ray: decreased joint space, osteophyte formation, sclerosis of femoral head, subchondral cysts • Treatment: NSAIDS for acute flare, Tylenol/NSAID for long-term analgesia • Physiotherapy: ROM, strengthening, gait aids • Partial/Total hip replacement
Avascular Necrosis • Etiology: Loss of vascular supply to femoral head • Primarily distal to proximal intra-osseous blood supply • Predisposing factors: systemic steroid, dislocation of femur, fracture of femoral neck, chronic alcohol use, sickle cell, septic arthritis, “the Bends”
Avascular Necrosis • Symptoms: Pain in groin, worse with WB • O/E: abnormal range of motion if collapse of cartilage on femoral head • Normal strength on manual muscle testing • Pain on compression testing • X-ray may show crescent sign • Treatment: Non WB until new bone formation
Trochanteric Bursitis • Etiology: trauma to hip, abnormal gait mechanics, muscle tightness, over-training • Rule out cellulitis or infection • Pain at lateral aspect of hip, worse with weight bearing/ walking/ direct pressure • O/E: pain on palpation over greater trochanter, +/- tight ilio-tibial band, muscle imbalance, pain on single leg stance
Trochanteric Bursitis • Treatment: Rest, Ice, NSAIDS • Physiotherapy for stretching, muscle imbalance • Consider corticosteroid injection for refractive conditions
FAI: Femoroacetabular Impingement of the Hip • Abnormal contact between the acetabulum and femoral head-neck junction • Primarily an impingement issue • Groin pain with activity or extreme ROM • Usually younger active people • Can lead to labral tears
Of the four muscles of the quadriceps, which crosses two joints? • Rectus femoris • Vastus lateralis
Muscle strains • Adductors: groin pull • Hip flexors: Rectus femoris strain • Snapping hip: iliopsoas • Piriformis syndrome • Iliotibial band syndrome • Gluteal strain