Download
1 / 33
640 likes | 2.59k Views
NERVE INJURIES. Dr. JOYCE DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY YDC. MAY OCCUR FOLLOWING. Mandibular and maxillary orthognathic surgery Maxillofacial trauma Dental implant placement Endodontic therapy Facial fractures Treatment of pathology

E N D
NERVE INJURIES Dr. JOYCE DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY YDC
MAY OCCUR FOLLOWING • Mandibular and maxillary orthognathic surgery • Maxillofacial trauma • Dental implant placement • Endodontic therapy • Facial fractures • Treatment of pathology • Third molar surgery is responsible for most of the injuries to both the inferior alveolar and lingual nerves
Mechanisms of Peripheral Nerve Injury • Laceration • Stretch injuries. • Pressure. • Nerve damage due to injections. • Chemical nerve injury.
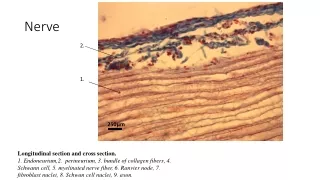
FUNCTIONAL HISTOLOGY OF THE PERIPHERAL NERVES • Peripheral nerves are complex structures consisting of fascicles held together by the epineurium – an enveloping, external connective sheath. • Endoneurium-consist of loose connective tissue with capillary blood vessels. • Perineurium-is a multilayered epithelial sheath that surrounds individual fascicles and consists of several layers of perineural cells. • fascicle is a group of nerve fibers surrounded by perineurium.
Fascicles can be organized in one of three common arrangements: • Monofascicular (single, large fascicle) • Oligofascicular (few fascicles of various sizes) • Polyfascicular (many fascicles of various sizes). • Inferior alveolar and lingual nerves are polyfascicular in nature.
oligofascicular monofascicular polyfascicular
Nerve injury classification: • Seddon :1943 • Sunderland : 1951
1953 SUNDERLAND CLASSIFICATION • First degree (neuropraxia): Electrical conduction is blocked but axoplasmic flow continues bidirectionally. • In neuropraxia, the distal aspect of the nerve retains normal electrical stimulability, but voluntary motor function is abnormal. • Usually neuropraxia is the result of a compressive lesion or mild trauma to the nerve during surgery. • Following neuropraxia, nerve function usually returns to normal after the offending compression or injury subsides.
SECOND-DEGREE (AXONOTMESIS): Axonal continuity is lost and wallerian degeneration sets in distally. In this type of injury, the proximal myelin sheath remains intact and the endoneurial sheaths are preserved. The prognosis following axonotmesis is good because of the preservation of the endoneurium, which helps channel the growing axons to the distal facial muscles. • THIRD DEGREE: The endoneurial tube is disrupted. • FOURTH DEGREE: The endoneurium and perineurium are disrupted and the fascicles are no longer segregated. • FIFTH DEGREE: The endoneurium, perineurium, and epineurium are disrupted.
Neuritis • Inflamation of nerve . • Causes : • Traumatic neuritis(when nerve is lacerated ) • Infectious neuritis. • Causes: • Herpes zooster • Toxic neuritis: • Arsenic,lead,mercury.
Clinical features: • Deep seated pain. • Diffuse and continious in character. • Functional loss is also seen when a motor nerve is involved. • Hyposthesia: decrease sensitivity to pain. • Anesthesia: total loss of all type of stimulation. • All these may may last for several weeks.
Treatment • Analgesics. • VIT B1 B6 B12. • Infra red lamps.
Neuroma: • Microspourting disorganised formation of disorganised mass of collagen and randomly oriented small fasciles. • Types : • Amputation neuroma. • Neuroma in continuity. • Lateral exophytic neuroma. • Lateral adhesive neuroma.
Treatment • Nerve inspection is done for identification of neuroma. • High magnification provides where to resect. • Beaver blade is used for resection. • Sharp resection is advisable. • 3mm proximal and distal to the neuroma should be resected along the neuroma.
Diagnostic evaluation of nerve injury • This includes a properly taken thorough HISTORY,CLINICAL EVALUATION and some diagnostic testing as NERVE blocks and ELECTROPHYSIOLOGICAL testing of nerve and muscles. The basic clinical examination involves testing for motor function, sensory function and autonomic function
Clinical evaluation: • Patients main complaint. • Patient’s history: • Trauma or surgical procedure. • Date of incidence. • Progress of symptoms or functional complaints
Signs and symptoms: • Nonpainful anesthesia, hypoesthesia, hyperthesia /painful anesthesia. • Numbness, crawling, stretched, painful, tingling, tickling, burning, pins and needles perception. • Inability to feel food, smile.
Aggravating ,releiving factors. • Visual analogous scale.
CLINICAL NEUROSENSORY TESTING • Level A testing includes brushstroke directional and static two-point discriminations. • Level B testing contact detection is performed with Semmes-Weinstein monofilaments or von Frey hairs.\ • Level C testing pinprick nociception and thermal discrimination
Nerve blocks • Nerve blocks can be given to differentiate between psycogenic pain and pain due to nerve injury . • Before administrating local anesthetic solution normal saline should be injected to act as an placebo. • Nerve block should proceed from proximal to distal .
MANAGEMENT MEDICAL SURGICAL
Medical management for pain: • Analgesics. • Anesthetics. • Antidepressants. • Antiepleptics .
Surgical • Indications: • Observed nerve injuries • Presence of foreign bodies • Unchanging anesthesia for more than 2 months • Failure of medical management
Contraindications: • Signs of nerve improvement . • Signs of central sensitization. • Extreme age • Excessive time • Medically compromised • Sensory deficit acceptable to patient.
Decompression • Removal of foreign bodies . • Impinging bone or tooth fragments. • Preserve vasculature of the nerve . • Investigation • Nerve continuity,neuromas. • Polyglycolic acid collagen neurocuffs. • Type 1, 2. nerve injury.
Neurorraphy • Act of bringing the nerve ends together and maintaining this position with sutures. • Direct neurorrhaphy. • Indirect neurorrhaphy
Direct neurorapphy • Epineural sutures . • No perineural sutures. • 7-0,9-0 nonabsorbable sutures. • No resorbable suture. • 2 sutures per anastomosis. • Not more than 3-4 sutures . • Medial first. • 0.5-1.0 mm bite. • 2nd 180 degree. Lateral aspect
Indirect neurrhaphy • Tension ,nerve gap exists in direct neurrhaphy procedure. • Grafting is considered. • Sural nerve, greater auricular nerve, medial antebrachial cutaneous nerve. • Sural nerve: • Matches nerve diameter and pattern. • Grafts 20 centimetresis possible with sural nerve.