Download
1 / 17
170 likes | 288 Views
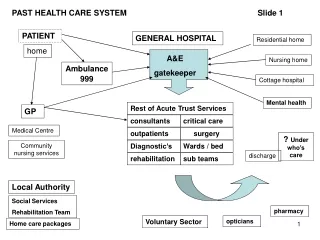
Kelowna General Hospital AMI IMPROVEMENT TEAM. Background. KGH – very busy 333 bed Tertiary Care facility, averaging 104% capacity 191 random AMI charts from Oct. 2004 to Oct. 2005 were audited by student nurses, and showed weaknesses in: Door to Thrombolytic time

E N D
Kelowna General Hospital AMI IMPROVEMENT TEAM Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Background • KGH – very busy 333 bed Tertiary Care facility, averaging 104% capacity • 191 random AMI charts from Oct. 2004 to Oct. 2005 were audited by student nurses, and showed weaknesses in: • Door to Thrombolytic time • Smoking cessation counseling/ interventions • AMI Team evolved in response to recommendations from this study Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Background • Multidisciplinary Team from a number of areas: Emerg, Critical Care, Cardiology, Cath Lab, Cardiac Rehab/Community, QI, Pharmacy, BCAS, Health Records, etc. • Recommendations acted upon: • Triage standing order for administering ASA and ordering diagnostics • EHS administers ASA in the field • ALS EHS perform 12 lead ECG in the field Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Background • Despite above modifications in practice, Avg. Time to Thrombolytic has not improved • Original Team experienced dissolution when Emerg Manager champion left job in early 2006. • New AMI Team formed in Jan. 2007 and charter written. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Aim Statements • Document goal of “Best Process of Care” by increasing percentage of patients receiving Perfect Care Measure by 10% by December 2007. • Increase percentage of patients receiving timely initiation of thrombolytics to 85% by Apr. 1, 2008. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Aim Statements • Increase percentage of smokers receiving smoking cessation intervention to 95% by Apr. 1, 2008. • Provide Quality Improvement AMI Initiative feedback to appropriate front line staff on a monthly basis. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Team Members • Physicians • Cardiologist • Nurse Managers • Clinical Nurse Educators/ Patient Care Coordinators • Bedside Nurses • Clinical Pharmacist • Respiratory Therapist • Cardiac Revascularization / Cardiac Rehab Coordinators • BCAS Rep • Quality Improvement (SHN) Rep Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Changes Tested • Concurrent audit tool (initiated by Triage RN, traveling with patient chart) developed and trialed • With incentive rewards • Without incentive rewards • Development/ implementation of STEMI/ NSTEMI order sets, following Best Practice guidelines (in progress) Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Changes Tested • Retrospective chart audits of patients receiving thrombolytics: • looked for variance from Best Practice • examined times of elements contributing to delay to thrombolytic i.e. times of: • Arrival • Triage • Bed • ECG • Physician exam • Thrombolytic administered Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results • Compliance with Triage Nurse initiating concurrent audit form was about 10%, with incentive rewards. Unfortunately staff compliance for completing the audit tool disappeared with the funding for rewards. • Concurrent audit forms were not always accurately completed. Sometimes information was entered that would reflect more favorably on department performance. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results • Bundle elements that were a problem two years ago remain a problem, i.e. • Door to Thrombolytic time • graph shows it is actually getting worse • Smoking cessation counseling/ interventions Limited data follows… Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Keys to Success and Lessons Learned • Good communications at all phases are imperative. Processes that take place without adequate input from all stakeholders fail to get buy-in. • Incentive rewards and compensation improve participation and compliance! • Chart audits are time consuming. It is a non-sustainable way of obtaining data. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Keys to Success and Lessons Learned • PDSA’s are most likely to succeed when there is a champion on the floor to engage staff, drive the process, and promote effective communications. • Difficult to do PDSA’s in understaffed/ grossly overcapacity ward or department. We have backed off working in ED until a project improving patient flow is completed. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Next Steps • Add more front-line nurse champions to team • Focus on ways to improve smoking cessation counseling and interventions • proposal has been submitted to Health Canada’s Tobacco Control Program • Re-focus on improving Time to Thrombolytic once flow of patients through ED has improved. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Contact Information • Sherri Ellis (Registered Nurse, Cardiology) ELLS@mox.interiorhealth.ca (250) 862-4232 • Karla Waller (Registered Nurse, Cardiology) WALK2@mox.interiorhealth.ca (250) 862-4232 • Holly Morgan (Clinical QI Coordinator) holly.morgan@interiorhealth.ca (250) 862-4300 Ext 7210 Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative