Download
1 / 47
470 likes | 1.36k Views
BRIEF ® : Behavior Rating Inventory of Executive Function ® Authors: Gerard A. Gioia , PhD, Peter K. Isquith , PhD, Steven C. Guy, PhD, and Lauren Kenworthy , PhD Publisher: PAR, Inc. BRIEF Authors. Gerard A. Gioia , Children’s National Medical Center

E N D
BRIEF®: Behavior Rating Inventory of Executive Function®Authors: Gerard A. Gioia, PhD, Peter K. Isquith, PhD, Steven C. Guy, PhD, and Lauren Kenworthy, PhDPublisher: PAR, Inc.
BRIEF Authors • Gerard A. Gioia, Children’s National Medical Center • Peter K. Isquith, Dartmouth Medical School • Robert M. Roth, Dartmouth Medical School • Steven C. Guy, Independent Practice • Lauren Kenworthy, Children’s National Medical Center • Kimberly Andrews Espy, Vice Provost, University of Nebraska, Lincoln
Overview of the BRIEF • Purpose: Assess impairment of executive function • For: Ages 5-18 years • Administration: Individual, 86 items • Time: 10-15 minutes to administer; 15-20 minutes to score by hand, software available for scoring and interpretation
Overview of the BRIEF • Utilizes parent and teacher input in the evaluation of the child’s behavioral functioning • The BRIEF is useful in evaluating children with a wide spectrum of developmental and acquired neurological conditions, such as: • Learning disabilities • Low birth weight • Attention-deficit/hyperactivity disorder • Tourette's disorder • Traumatic brain injury • Pervasive developmental disorders/autism
Interest in Executive Function in Children • 5 articles in 1985 • 14 articles in 1995 • 501 articles in 2005 • Bernstein & Waber, Executive Function in Education, 2007
Methods of Assessing EF Macro Micro Structural & Functional Imaging Performance Tests Genetics Observations
Measurement of Executive Functions • Executive functions are dynamic, fluid • No formal, single test adequate to capture EF • Many tests are too structured to adequately assess EF • Need intra-individual approach • “Executive” is often provided by the examiner
Limitations of Performance Tests • EF tests are molar, tapping several EF and non-EF functions that can be disrupted in many ways • Differences in cognitive “style” or ability can affectEF performance regardless of EF • Sensitivity/Specificity limited − Patients who should have EF deficits do well on EF tests; EF performance not sensitive to frontal vs. extra-frontal lesions • Discriminant Validity − If EF tasks are impaired in several disorders, then EFs are not helpful in distinguishing between disorders • Pennington & Ozonoff, 1996
Impetus • Clinical need for efficient external validation • Collect standardized observational reports of everyday functioning • Ecological validity, real-world anchor • Common parent descriptions of everyday executive difficulties • Frustration with available performance tests
Purpose: provide a measure of executive function that is: • psychometrically sound • sensitive to developmental changes • high in ecological validity • sufficiently broad to serve as a screen • comprehensive in sampling content • theoretically coherent • useful in targeting treatment
Purpose of the BRIEF • The BRIEF consists of two rating forms • Parent • Teacher • 86 items on both questionnaires
Additional BRIEF Products • BRIEF Preschool (Ages 3-5 years) • BRIEF Self-Report (Ages 13-18 years) • BRIEF Software (Scoring & Reporting) • BRIEF Adult (Ages 18-90 years)
A BRIEF Genealogy 2000 2003 2004 2005
Meta- Cognition Monitor Organizationof Materials Plan/Organize Working Memory Initiate Behavioral Regulation Emotional Control Shift Inhibit
Behavioral Definitions for the Clinical Scales • Inhibit: Control impulses; stop behavior • Shift: Move freely from one activity/situation to another; transition; problem-solve flexibly • Emotional Control: Modulate emotional responses appropriately
Behavioral Definitions for the Clinical Scales • Initiate: Begin activity; generate ideas • Working Memory: Hold information in mind for purpose of completing a task • Plan/Organize: Anticipate future events; set goals; develop steps; grasp main ideas • Monitor: Check work; assess own performance
Administering the BRIEF Parent Form • Materials: Parent Form and a pen/pencil • Parent Form is filled out by a parent; preferably, by both parents • Parent must have recent and extensive contact with the child over the past 6 months
Administering the BRIEF Teacher Form • Can be filled out by any adult with extended contact with the child in an academic setting; typically a teacher, but an aide is acceptable • Minimum familiarity is 1 month • Multiple ratings across classrooms may be useful for comparison purposes
Scoring the BRIEF Parent/Teacher Forms • Calculate the raw score by transferring the circled responses to the box for that item • Sum the scores in each column and record the sum in the box for that column • Transfer the summed scores from page 1 to the appropriate box on page 2 and then sum the scores for each scale
Scoring the Negativity Scale • To score the Negativity scale, find all of the “N” items that received a score of 3 • Sum the number of “N” items that received a score of 3 and record that number in the Negativity scale box in the Scoring Summary/Profile Form
Scoring the Inconsistency Scale • Scoring the Inconsistency scale is more complex and requires greater attention to detail • Inconsistency items have an I in the margin of the scoring sheet • Transfer the scores for the 10 item pairs to the appropriate boxes on the Scoring Summary/Profile Form
Scoring the Inconsistency Scale • For each item pair, calculate the absolute value of the difference for the items • Then, sum the difference values for the 10 pairs to obtain the Inconsistency scale score
Obtaining Standard Scores for the BRIEF Parent/Teacher Forms • Once raw scores for all scales are obtained, find the appropriate table in the appendixes • Tables are broken down by form (Parent/Teacher), age, and gender ofthe child • Standard scores have a mean of 50 and a SD of 10; percentile ranks also are available in the tables
Comparison Tables • Separate normative tables for both the Parent and Teacher Forms provide T scores, percentiles, and 90% confidence intervals for four developmental age groups (5-18 years) by gender of the child
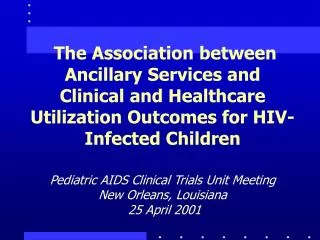
Joshua ADHD - Combined Type
Computerized Scoring • BRIEF Software Portfolio (BRIEF-SP) provides unlimited scoring and report generation for the BRIEF Parent Form, the BRIEF Teacher Form, the BRIEF-SR, the BRIEF-P Parent Form, and the BRIEF-P Teacher Form. Three reports are available − an Interpretive Report, a Feedback Report, and a Protocol Summary Report. • Separate software is available for the BRIEF-P only and the BRIEF-A only.
Interpreting the BRIEF Parent/Teacher Forms • All results should be viewed in the context of a complete evaluation • High scores do not indicate “A Disorder of Executive Function” • Problems may be developmental or acquired and, thus, are suggestive of differing treatment approaches
Steps to BRIEF Interpretation • Examine validity scales • Inconsistency • Negativity • Examine clinical scales • Examine indexes, Global Executive Composite • Individual item analysis • Within scale items • Nonscale items
Interpretation • T scores at the Domain level; higher scores suggest a higher level of dysfunction • For the Inconsistency scale, look at scores ≥7 as indicative of a high degree of inconsistency in rater response • A high Negativity scale score indicates the degree to which the respondent answers selected questions in an unusually negative manner. “Is information consistent with other sources?”
Interpretive Options • Professional Manual • Computer Scoring and Interpretive Reporting • Integrated Reporting
Reliability • High internal consistency (α = .80-.98) • Test-retest reliabilityrs = .82 for parents and .88 for teachers; moderate correlations between teacher and parent ratings (rs = .32-.34)
Validity • Convergent validity established with other measures: inattention, impulsivity, and learning skills • Divergent validity demonstrated against measures of emotional and behavioral functioning • Working Memory and Inhibit scales differentiate among ADHD subtypes
Standardization Population • Normative data based on child ratings from 1,419 parents and 720 teachers from rural, suburban, and urban areas, reflecting 1999 U.S. Census estimates for SES, ethnicity, and gender distribution
Clinical Standardization Population • Clinical sample included children with developmental disorders or acquired neurological disorders (e.g., reading disorder, ADHD subtypes, TBI, Tourette's disorder, mental retardation, localized brain lesions, high functioning autism)
Diagnostic Group Studies • Reading Disorders • Working Memory: Reading > Controls • Plan/Organize: Reading > Controls • B. Pratt, F. Campbell-LaVoie, P. Isquith, G. Gioia, & S. Guy • Extremely Low Birth Weight vs VLBW • Monitor, WM, Shift, Inhibit, Init, Plan/Org: ELBW > Controls • Initiate & Plan/Org: ELBW > VLBW • G. Taylor, et al. • Mental Retardation • Working Memory: MR > Controls • B. Pratt & T. Chapman
Diagnostic Group Studies • High Functioning Autism • All BRIEF scales: HFA > Controls • R. Landa & M. Goldberg • Pervasive Developmental Disorders • All BRIEF scales: PDD > Controls • L. Kenworthy & S. Guy • Frontal vs. Extrafrontal Lesions • All scales: Frontal & Extrafrontal > Controls • Inhibit: Frontal > Extrafrontal > Controls • R. Jacobs, V. Anderson, & S. Harvey
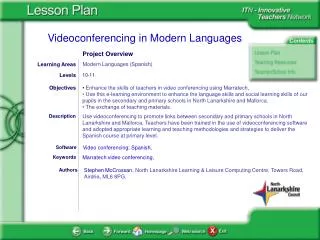
Case Example • Joshua: • 8-year-old left-handed male • Attention-Deficit/Hyperactivity Disorder, Combined Type
Joshua ADHD - Combined Type
Joshua ADHD - Combined Type
BRIEF Clinical Studies • ADHD - Jarratt et al., 2005; Loftis, 2005; Viechnicki, 2005; Lawrence et al., 2004; Blake- Greenberg, 2003; Palencia, 2003; Kenealy, 2002; Mahone et al., 2002. • Reading disorders- Gioia et al., 2002; Pratt, 2000. • Autism spectrum disorders- Gilotty et al., 2002; Gioia et al., 2002. • Bipolar disorder vs. ADHD- Shear et al., 2002. • Tourette’s syndrome- Mahone et al., 2002; Cummings et al., 2002. • Traumatic brain injury - Landry et al., 2004; Brookshire et al., 2004; Gioia et al., 2004; Mangeot et al., 2002; Vriezen et al., 2002; Jacobs, 2002. • Media violence exposure -Kronenberger et al. 2005. • Spina bifida and hydrocephalus - Burmeister et al., 2005; Brown, 2005; Mahone et al., 2002. • Obstructive sleep apnea -Beebe, 2004, 2002. • Galactosemia- Antshel et al., 2004. • Childhood onset MS -McCann et al., 2004. • Sickle cell- Kral et al., 2004. • 22q11 deletion - Kiley-Brabeck, 2004. • PKU - Antshel et al., 2003. • Frontal lesions, PKU & hydrocephalus - Anderson et al., 2002.