Download
1 / 28
400 likes | 1.37k Views
Proximal Humerus Fractures ORIF & Arthroplasty. Reza Omid, M.D. Assistant Professor Department of Orthopaedic Surgery Keck School of Medicine of USC. Introduction. 5-7% of all fractures 80% treated nonoperatively (Neer) Bimodal incidence

E N D
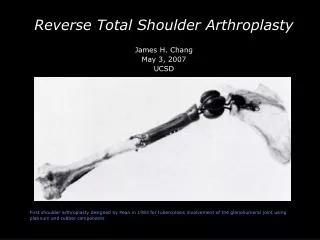
Proximal Humerus Fractures ORIF & Arthroplasty Reza Omid, M.D. Assistant Professor Department of Orthopaedic Surgery Keck School of Medicine of USC
Introduction • 5-7% of all fractures • 80% treated nonoperatively (Neer) • Bimodal incidence • Bone quality- important factor in obtaining secure fixation
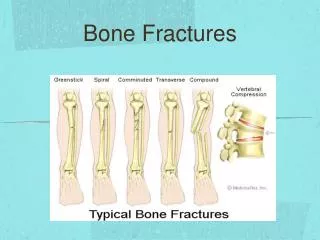
Proximal Humeral Anatomy Understanding Fracture Patterns • 4 bony fragments • Lesser Tub • Greater Tub • Head • Shaft Neer, JBJS ‘70
Proximal Humerus Fractures Fracture Patterns • Stable • Fx not controlled by muscle • Unstable • Fx controlled by attached muscle
Proximal Humerus Fracture Fracture Anatomy • Greater Tub – posterior, proximal • Lesser Tub – medial, inferior • Head – remaining tub or fx energy • Shaft – medial, superior
Proximal Humerus Fracture Fracture Anatomy
Consideration for Surgery Bone Quality Comorbidities Functional demand Vascularity???
Gerber JBJSAm 1990: 1486-94 Vascularity • anterior humeral circumflex • Anterolateral branch Of AHC (arcuate artery) Along lateral aspect of groove
Brooks JBJSBr 1993: 132-136 • Vascularized through interosseous anastomoses • Between metaphyseal vessels (via posterior humeral circumflex) and the arcuate artery after ligation of the anterior circumflex humeral.
Coudane JSES 2000: 548 • Arteriography done on 20 patients after proximal humerus fractures. • 80% had disruption of AHC artery • 15% had disruption of PHC artery • Since AVN is rare (bw 1-34%) after fx it suggests the PHC artery may be dominant supply
Hettrich JBJSAm 2010: 943-8 • MRI cadavers • posterior humeral circumflex • supplied 64% of head (superior, lateral and inferior).
Hertel Criteria Hertel et al JSES 2004:13:427 • Medial calcar segment <8mm • Medial hinge is disrupted (>2mm displacement of the diaphysis) • Comminution of the medial metaphysis • Anatomic neck fracture
Bastian JSES 2008: 2-8 • Follow-up study by Hertel showed that initial predictors of humeral head ischemia doesn’t predict development of AVN. • 80% of patients with “ischemic heads” did NOT collapse • Fixation is worth considering even if signs of ischemia are present
Nonoperative Treatment Immobilize initially Passive ROM 2-3 weeks • supine FE • supine ER • pendulums AROM at 6 weeks or when consolidated 77% good to excellent results-Zuckerman 1995
Optimal Treatment • UNKOWN???? • JSES 2011: 1118-1124 (RCT ORIF vs Non-op) • JSES 2011: 747-55 (RCT ORIF vs Non-op • JSES 2011: 1025-1033 (RCT Hemi vs Non-op) • JOT 2011 (RCT ORIF vs Non-op)
Three-Part Fractures Fixation Options • Percutaneous Pins • Interfragmentary Suture/Wire • Plate/Screws • IM Nail • Blade Plate • Hemiarthroplasty
Reduction & Grafting • Impaction grafting of head • Iliac crest cube • Fibular strut
Four precise holes for medial calcar support that provide a stable fixation in the calcar neck while preventing varustilt and settling of the humeral head Proximal Screws angle towards posterior portion of humeral head to take advantage of the good bone quality of the posterior portion 3.5mm locking screw holes establish a stable bone and plate construct 3.5mm partially threaded screw options allow for compression of fragments and ability to pull the head fragments into reduction Polished suture holes allow for soft tissue and tuberosity fixation Humeral Fracture Plates 23
Restore the calcar! • “Medial comminution significantly decreased the stability of proximal humeral fracture fixation constructs. Calcar restoration with screw fixation significantly improved the stability of repaired fractures in cadaveric specimens.” DePuy/SynthesPhilos Plate – only 2 calcar screw holes Fig. 1Figs. 1-A through 1-E Radiographs and diagram illustrating the fracture models and fixation constructs used. Fig. 1-A Medial comminution without calcar fixation. Fig. 1-B Noncomminuted fracture without calcar fixation. Fig. 1-C Medial comminution with calcar fixation. Fig. 1-D Noncomminuted fracture with calcar fixation. Fig. 1-E Diagrammatic illustration of the PHILOS plate. Ponce BR. The Role of Medial Comminution and Calcar Restoration in Varus Collapse of Proximal Humerus Fractures Treated with Locking PlatesJ Bone Joint Surg Am, 2013 Aug 21;95(16):e113 1-7. doi: 10.2106/JBJS.K.00202
Proximal humeral fractures: Regional differences in bone mineral density of the humeral head affect the fixation strength of cancellous screws Implant loosening as a result of poor bone quality is a serious complication after internal fixation of displaced fractures of the proximal humerus. investigated the relationship between trabecular BMD and the pullout strength of cancellous screws to determine regions in the humeral head that provide stronger fixation for cancellous screws. trabecular BMD of the humeral head has a significant effect on the pullout strength of cancellous screws. Central and posterior regions are best. Avoid superior-anterior region. Tingart et al, JSES 2006
Designed to sit lower on the greater tuberosity Removed the 2.7mm screw holes Minimizing subacromial impingement Thinner design to reduce soft tissue irritation 4-point bending was completed Results show LP Plate is stronger than the predicate plate (Synthes) 4 Medial Calcar “kick stand” screws to prevent varus tilt/settling of humeral head Anatomic fit with right and left plates and different length plates 3-hole (89mm) 6-hole (112mm) 9-hole (135mm) Made from 316L Stainless Steel Low Profile Plate Design November 20, 2011 26
6 proximal suture holes for soft tissue/tuberosity fixation Easy in-situ needle passing through angled and scalloped holes Also used as wire holes for initial plate fixation 4 Proximal 3.5mm screw holes Utilizing locking or compression screws 5 Calcar 3.5mm screw holes Utilizing locking or compression screws Parallel in AP view 3o divergence in S/I view and Lateral view Distal 3.5mm screw holes Utilizing locking or compression screws Compression slot utilizing compression screws Low Profile Plate Specifications November 20, 2011 27
Conclusions • Best to perform repair for acute fracture • Anatomic restoration of humeral height and version • Secure tuberosity fixation • Repair the cuff • Tenodesis of the LHB • Early protected PROM, close supervision of the rehabilitation program