Download
1 / 36
360 likes | 404 Views
Osteoporosis is a skeletal disease characterized by low bone mass, leading to increased fracture risk. Learn the diagnosis, pathophysiology, and consequences of osteoporosis, particularly in postmenopausal women. Discover the impact on morbidity and mortality associated with this underestimated disease.

E N D
Osteoporosis an underestimated disease
Definition of osteoporosis …a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue leading to enhanced bone fragility and a consequent increase in fracture risk. World Health Organization (WHO). Technical Report Series 843, Geneva 1994Update TRS 921, 2003
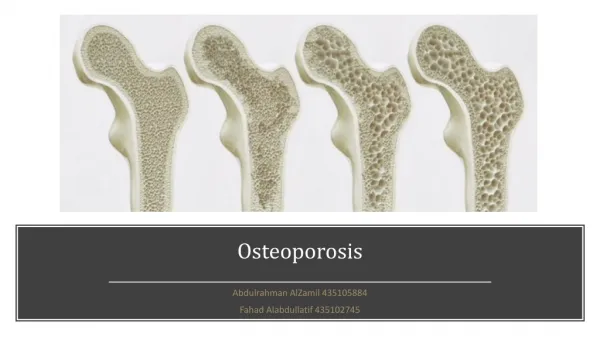
normal osteoporotic
Osteoporosis diagnosis Areal bone mineral density is a important predictor of fracture risk. Spine/hip dual energy X-ray absorptiometry measurement (DEXA) is the diagnostic standard WHO. Technical Report Series 921, Geneva 2003
Dual Energy X-ray Absorptiometry or DEXA • Measures X-ray absorption • Bone mass per projected area (g/cm2) • BMD correlates with whole bone strength Bouxsein ML, et al. Bone 1999; 25(1):49-54.
BMD T-score=number of SD vs. mean BMD of healthy young female population (at peak bone mass) WHO, 1994 – update 2003
DEXA as BMD-measurement method Peak Bone Mass Osteoporosis Normal Osteopenia 0 –1 –2 –2.5 T-score DEXA = Dual-Energy X-ray Absorptiometry
‘Established osteoporosis’ WHO criteria for osteoporosis in women World Health Organization (WHO). Technical Report Series 843, Geneva 1994Update TRS 921, 2003
Diagnosis of Osteoporosis • BMD T-score -2.5 DEXA and / or • presence (history) of osteoporotic fracture RX
Osteoblast Osteoclast imbalance of bone-remodeling Age 40 Age 60 Age 70 Progression of vertebralfractures in osteoporosis
1989 1996 1959 Inger Lundegaardh, Sweden IOF: international osteoporosis foundation, http://www.osteofound.org
Pathophysiology of osteoporosis:bone remodelling Lining cells cover resting bone Osteoclasts resorb bone Activation resorption phase ~20 days Bone Bone Osteoblasts lay new osteoid Reversal formation phase ~160 days Bone Bone Newly laid osteoid mineralises overseveral months
Postmenopausal bone loss: role of estrogen deficiency Indirect effects Estrogen deficiency Dietary calcium(decreased absorptiondue to Vit. D deficiency) ? Directly increasesosteoclast number and longevity Decreased bone formation Secondary hyperparathyroidism Increased bone resorption Remodelling imbalance Bone Loss Adapted from Riggs BL, et al. J Bone Miner Res 1998; 13(5):763-773.
Age-related bone lossoccurs in men and women I Men I III Women II Bone mass III I Peak bone mass II Rapid bone loss (menopause)III Age-related bone loss 0 20 40 60 80 100 Age (years)
Bone Remodelling throughout Life Bone turnover = a coupled process always : bone resorption → bone formation • Childhood & adolescence: resorption < formation • As from the age of 40: resorption > formation • always negative balance per bone remodelling cycle • slow bone loss • Postmenopausal period: accelerated bone loss • estrogens inhibit bone turnover • E-deficiency → higher bone turnover rate
Low TURNOVER = low BONE LOSS High TURNOVER = high BONE LOSS Pathogenesis of Osteoporosis > 40 y negative net balance per bone remodelling cycle
Distribution of trabecular and cortical bone throughout the skeletal system Femoral neck25% trabecular75% cortical Vertebrae66% trabecular34% cortical Forearm(distal radius)20% trabecular80% cortical Trochanteric region50% trabecular50% cortical adapted from http://www.merckmedicus.com
Incidence of osteoporotic fractures in women Vertebrae Annual incidence Hip Wrist 50 60 70 80 Age (years) Adapted fromWasnich RD, Osteoporos Int 1997;7 Suppl 3:68-72and Sambrook P et al. Lancet 2006; 367(9527):2010-2018
Lifetime fracture risk of people at 50 years of age Adapted from Melton LJ, III, et al. J Bone Miner Res 1992; 7(9):1005-1010. .
All fractures are associated with morbidity One year after a hip fracture Unable to carry out at least one independent activity of daily living 80% Patients (%) Unable to walk independently Discharged toNursing Home 40% Death within one year 30% ≥20% Adapted from Cooper C. Am J Med 1997; 103(2A):12S-17S.
Morbidity after vertebral fractures • Back pain • Loss of height • Deformity (kyphosis, protuberant abdomen) • Reduced pulmonary function • Diminished quality of life: loss of self-esteem, distorted body image, dependence on narcotic analgesics, sleep disorder, depression, loss of autonomy, social dependence • Increased mortality http://www.osteofound.org/
Age-Standardized Mortality Ratio FractureWomen Men Proximal femur 2.2 3.2 Vertebral 1.7 2.4 Other major 1.9 2.2 Minor 0.8 1.5 Mortality after major types of osteoporotic fracture in men and women 5 - Year Prospective Cohort Study Adapted from Center JR, et al. Lancet 1999; 353(9156):878-882..
Economic Impact Number of bed days (men and women)in Switzerland in 1992: 701,000 for osteoporosis 889,000 for chronic obstructive pulmonary disease 533,000 for stroke 328,000 for myocardial infarction 201,000 for breast cancer Osteoporosis # 1 when looking at women only Adapted fromLippuner K, et al. Osteoporos Int 1997; 7(5):414-425.
Risk factors that provide indications for the diagnostic use of bone densitometry • Presence of strong risk factors • Previous fragility fracture • Radiographic evidence of osteopenia or vertebral deformity or both • Loss of height, thoracic kyphosis(after radiographic confirmation of vertebral deformities) Kanis JA. Lancet 2002; 359(9321):1929-1936.
Risk Factors that identify people who should be assessed* for Osteoporosis Minor Risk Factor Major Risk Factors • Age 65 years • Vertebral compression fracture • Fragility fracture after age 40 • Family history of osteoporotic fracture(esp. maternal hip fract.) • Systemic glucocorticoids (> 3 m) • Early menopause (before 45) • Malabsorption syndrome • Primary hyperparathyroidism • Propensity to fall • Osteopenia apparent on x-ray film • Hypogonadism • High Bone Turnover • Major immobility • Rheumatoid Arthritis • Hyperthyroidism • Anticonvulsant therapy • Chronic heparin therapy (UFH) • Calcium Intake < 500 mg/d • Smoking • Excessive alcohol intake • BMI < 19 * BMD measurement is recommended for those with at least 1 major or 2 minor risk factors . Adapted from Brown JP, et al. CMAJ 2002; 167(10 Suppl):S1-34.
Who to test (BMD-measurement) for Postmenopausal Osteoporosis ? • post-menopausal, 65 y • post-menopausal, < 65 y • with additional risk factors, or • with fragility fracture, or • with loss of height or deformity of the spine (kyphosis) • pre- or post-menopausal • with disease or receiving a treatment, known that they can cause a ‘secondary’ form of osteoporosis Adapted from Raisz LG. N Engl J Med 2005; 353(2):164-171.
Preventing osteoporosis C alcium D Vitamin E xercise F Prevent alls G ain weight S Stop moking
TREATMENT of OSTEOPOROSISin order to prevent (new) fractures
Strontium ranelate Drugs used in osteoporosis treatment • HRT • SERM/Raloxifene • Calcitonin • Bisphosphonates-Alendronate- Risedronate- Ibandronate • Parathyroid hormone Inhibition of resorption Stimulation of formation