Download
1 / 33
350 likes | 1.21k Views
Acid-Base Imbalance. Metropolitan Community College Fall 2013. Acid Base Balance. Hydrogen ions - Low concentrations but highly reactive Concentration affects physiological functions Alters protein and enzyme functioning Can cause cardiac, renal, pulmonary abnormalities

E N D
Acid-Base Imbalance Metropolitan Community College Fall 2013
Acid Base Balance • Hydrogen ions - Low concentrations but highly reactive • Concentration affects physiological functions • Alters protein and enzyme functioning • Can cause cardiac, renal, pulmonary abnormalities • Alters blood clotting, • Metabolization of meds
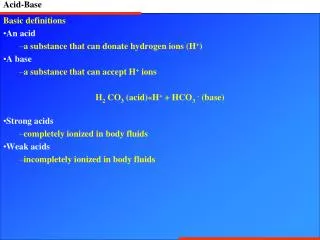
Acid and Bases • Acids – compounds that form hydrogen ion in a solution • Proton donors • Strong acids give up their hydrogen ion easily • Weak acids hold on to their hydrogen ion more tightly • Bases – compounds that combine with hydrogen ion in a solution • Proton acceptors • Neutralizes • 20:1 ratio (20 parts bicarbonate to one part carbonic acid)
What is pH? • pH is a measurement of the acidity or alkalinity of the blood. • It is inversely proportional to the number of hydrogen ions (H+) in the blood. • The more H+ present, the lower the pH will be. • The fewer H+ present, the higher the pH will be. • Homeostasis keeps pH in a very narrow range • 7.35-7.45 for optimum functioning • 6.8-7.8 compatible with life
Blood pH Blood pH < 7.40 acidosis Blood pH > 7.40 alkalosis
Body Acids • Respiratory Acid - CO2 – eliminated by lungs (288 L/day) • Metabolic acids: • Lactic acids • Pyruvic acid • Ketoacids (DKA) • Acetoatic acids • Beta-hydrobutyric acids • Very little metabolic acid is produced on a daily basis • Metabolized by the liver or eliminated by the kidneys
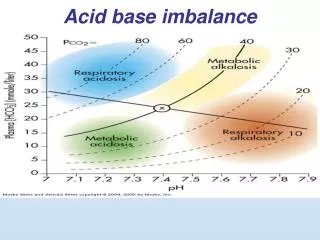
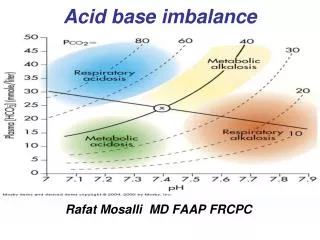
Four Basic Categories of Abnormalities • Respiratory acidosis • Excess of carbon dioxide leading to an acid pH • Respiratory alkalosis • Lower than normal level of carbon dioxide leading to an alkaline pH • Metabolic acidosis • Excess of hydrogen ion or a deficiency in bicarbonate leading to an acid pH • Metabolic alkalosis • Excess of bicarbonate leading to an alkaline pH
Buffer Systems • Like a sponge • Soaks up extra ions • Squeezed when there’s not enough • Extracellular Buffers • Carbonic acid: controlled by respiration • Bicarbonate: controlled by excretion • Intracellular Buffers • Phosphate Buffer System • Dihydrogen phosphate (H2PO4) – hydrogen donor or acid • Hydrogen phosphate (HPO4) – hydrogen acceptor or base
Buffer Systems • Protein Buffers • In the blood • Plasma Proteins • Hemoglobin: deoxygenated is better than oxygenated at buffering • Bones • Carbonate and phosphate salts in bone provide a long term supply of buffer. • In acute metabolic acidosis bone takes up hydrogen in exchange for calcium, sodium, and potassium.
Role of the Lungs • Regulate plasma pH minute to minute by regulating the level of Carbon Dioxide (CO2) • Carbon Dioxide is measured as a partial pressure of carbon dioxide in arterial blood • PaCO2 35-45mmHg • Lungs alter rate and depth of ventilations in order to retain or excrete CO2
Minute Volume – Tidal Volume • Ventilation is measured by how much air the lungs move in one minute (minute ventilation) • Minute Ventilation is the product of respiratory rate and depth and is referred to as the TIDAL VOLUME (Vt) • Normal depth tidal volume is about 500ml • Normal respiratory rate is 12 breaths per min 12 breaths x 500 ml = 6000 ml or 6 liters
Anatomic Dead Space • The volume of air that doesn’t reach the alveolar airspace • Trachea & Bronchi • Doesn’t take part in gas exchange • Estimated at 1ml/lb of ideal body weight • 150lb of ideal body weight = 150ml of dead space • Tidal volume – dead space = alveolar volume • 500ml – 150ml = 350ml • RR x alveolar volume = minute alveolar ventilation • 12 x 350ml = 4200ml or 4.2 L/min
Hypercarbic Drive • Respiratory center in the medulla controls the rate and depth of ventilation • Responds to levels of arterial CO2, denoted as PaCO2 • Chemoreceptors in the medulla come into contact with CSF • As PaCO2 rises the arterial PaCO2 reaches equilibrium with the CO2 in the CSF • The CO2 in the CSF dissociates into hydrogen ions • The hydrogen ions stimulate the chemoreceptors in the medulla which in turn stimulates the diaphragm and intercostal muscles • Respiratory rate and depth increase and CO2 is blown off
Hypoxic Drive • There are also peripheral chemoreceptors • Carotid arteries • Bifurcation of the common carotid and arch of aorta • Respond to levels of • Oxygen in the blood or PaO2 • Hydrogen ions or pH • Carbon dioxide in the blood or PaCO2 • As PaO2 falls below 60 mmHg the respiratory center is stimulated to increase rate and depth
The role of the Kidneys • Two main functions to maintain acid/base • Secrete hydrogen ions • Restore or reclaim bicarbonate (HCO3) • In high metabolic acidosis, the kidneys can excrete ammonia as a urinary buffer. • In alkalosis - the kidneys retain hydrogen ion and excrete bicarbonate to correct the pH. • In acidosis - the kidneys excrete hydrogen ions and conserve bicarbonate to correct the pH. • Very slow process
Assessment of ACID BASE • Arterial Blood Gases (ABG) most often and the most accurate to assess acid base balances. • Serum Electrolytes can help fine tune acid base analysis • NORMAL ABG VALUES: • pH = 7.35 to 7.45 • PaCO2 = 35 – 45 mEq/L • HCO3 = 22 – 28 mEq/L
Steps to Interpret ABG’s • Assess the pH • Assess the respiratory component – PaCO2 • Assess the metabolic component – HCO3, base excess • Evaluate compensation
Compensation • Once the primary cause is identified look at the other value • If the value is abnormal but moving in the right direction to bring pH back to normal compensation is occuring • If the pH value is normal than compensation is complete • Because renal compensation is slower you can infer whether respiratory abnormalities are acute or chronic • If kidneys have had time to compensate is chronic • If the kidneys have not had time to compensate its acute
Respiratory Acidosis • Respiratory system fails to keep up with the body’s CO2 production • Causes (pg. 442) • Acute: drug overdose, head trauma, spinal cord injury, upper airway obstruction, pneumothorax • Chronic: obesity, MS, emphysema, spinal cord injury • Clinical Manifestations • Anxiety, irritability, confusion, lethargy, increased heart rate, warm flushed skin • Mainly seen with acute causes because chronic patients have compensated
Respiratory Acidosis • Medical treatment • Treat the underlying problem • Increase ventilation • BiPAP • Intubation • Supplemental oxygen (care must be taken with chronic pts) • Nursing care • Assess PaCO2 levels and pH. • Observe for signs of respiratory distress: restlessness, anxiety, confusion, tachycardia • Encourage fluid intake • Position patients with head elevated 30 degrees • Administer oxygen with care
Respiratory Alkalosis • Most common cause is hyperventilation caused by anxiety, panic, or pain • Stroke • Meningitis • Head trauma • Clinical Manifestations • Anxious • Tachycardia • Tachypnea • Vertigo • Forgetfulness
Respiratory Alkalosis • Medical treatment • Treat underlying cause of condition • Sedation may be needed • Nursing care • Administer sedatives or pain medications • Provide emotional support • Encourage patient to breathe slowly, which will retain carbon dioxide in the body • Breath into a paper bag
Metabolic Acidosis • Increase in total body acid • Causes (pg. 442) • Starvation • Diarrhea • Renal failure • Diabetic ketoacidosis • Signs and symptoms • Kussmaul respirations • Altered LOC • Headache • V tach
Metabolic Acidosis • Medical treatment • Treat the underlying disorder • Nursing care • Monitor VS & ECG • Assess neurological status • Provide emotional support
Metabolic Alkalosis • An accumulation of base or a loss of acid in the ECF • Causes (pg. 442) • Prolonged nasogastric suctioning or excessive vomiting • Diuretics • Electrolyte disturbances • Large volume blood transfusions, increased citrate • Clinical Manifestations • Lethargy • Altered LOC • Tetany • ECG changes
Metabolic Alkalosis • Medical Treatment • Treat the underlying disorder • Nursing care • Monitor VS & ECG • Monitor labs • Accurate I&O including the amount of fluid removed by suction • Provide emotional support • Use isotonic saline solutions rather than water for irrigating NG tubes because the use of water can result in a loss of electrolytes
A client’s blood gas results are pH 7.36, PaCO2 50, HCO3 30. What do these results indicate to the nurse? • Respiratory acidosis, compensated • Metabolic acidosis, compensated • Metabolic acidosis, uncompensated • Respiratory acidosis, uncompensated
Reference • Osborn, Wraa, & Watson chapter 19