Download
1 / 15
150 likes | 273 Views
MSH2 promoter study. MSH2 and MSH6. A Brief History. Two patients (SR and NM) were referred for MSH6 testing. Both patients were previously screened for MSH2 mutations – both negative. Both patients were RER +ve SR – BAT25 and BAT26 NM - BAT25, 26, 40 and D2S123

E N D
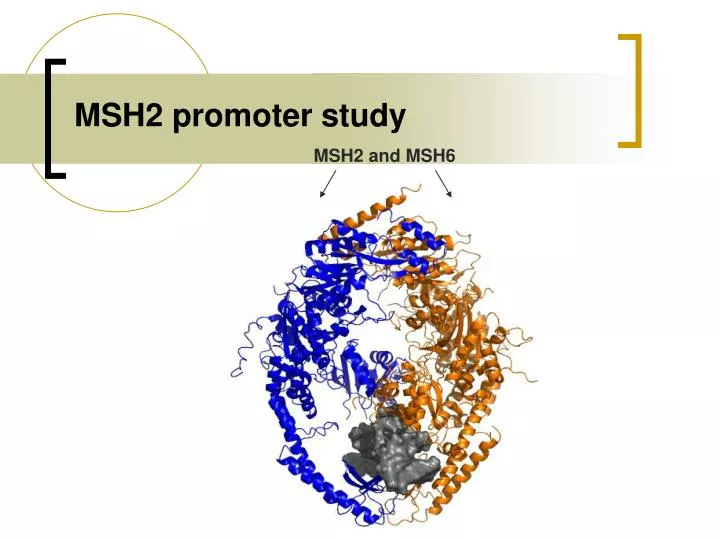
MSH2 promoter study MSH2 and MSH6
A Brief History • Two patients (SR and NM) were referred for MSH6 testing. • Both patients were previously screened for MSH2 mutations – both negative. • Both patients were RER +ve • SR – BAT25 and BAT26 • NM - BAT25, 26, 40 and D2S123 • Both patients showed loss of MSH2 by IHC. • NM had additional loss of MSH6 and PMS2
MSH6 mutation screen • Usual screening procedure. • Bi-directional sequencing. • MLPA • Both patients were normal and had no mutations other than neutral polymorphisms in MSH6 and no deletions were identified.
However, • The MSH6/PMS2 MLPA kit also contains additional probes. These include; • APC ex 7 • MLH1 ex 1 • MutYH exons 1, 2, 3, 14, & 16 • TACSTD1 ex 9.
MSH6/PMS2 (P008) MLPA TACSTD1 ex9 was sequenced and no polymorphisms were found under the probe ligation site.
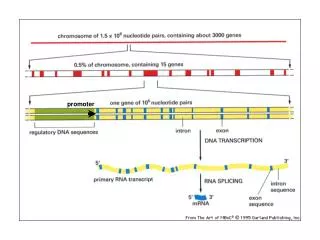
What could it mean? • This region chromosome 2p is very repetitive. • Previous studies have shown deletions within the coding region of MSH2 that extend to the promoter region and as far as the TACSTD1 gene.Francoise Charbonnier et al, HUMAN MUTATION 26(3), 255-261,2005 • Recombination between Alu elements have also been shown (ex1-ex6).Anja Wager et al., Am J. Hum. Genet.72:1088-1100,2003 • Could the apparent deletion in TACSTD1 ex9 extend into the promoter of MSH2?
Possible methods to test this? • Microarray – not high enough resolution. • Sequencing – deleted regions are not well characterised and could be as far as 15kb. • Dosage analysis • MRC Holland are working on introducing more probes into the MSH2 promoter region in the P008 kit, but they are not ready yet. • Settled on an “in-house” dosage assay.
MSH2 promoter dosage assay • QF-PCR based strategy • Multiplex of 15 primer combinations • Primer locations designed look specifically at the promoter but extend upstream into the TACSTD1 gene.
MSH2 promoter dosage assay • Used Primer3 to design primers in the usual fashion and product sizes were selected for a multiplex PCR. • Invitrogen Fw and Rv primers ordered and optimised on a gradient. • Fragments were sequenced to confirm their location within the promoter region. • ABI Fw primers were ordered with 6-FAM, NED and VIC fluorescent tags.
ABI analysis • Initially the dosage analysis was carried out on Normal control samples and a positive control sample (MSH2ex1 deletion that extends to TACSTD1 ex9). • PCR primer concentrations were optimised empirically.
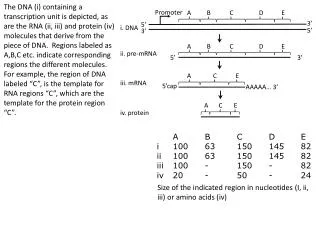
Dosage analysis 23.4Kb 15.2Kb 4.3Kb 2.4Kb 0.4Kb 17.9Kb 11Kb 3.7Kb 0.8Kb start Patient NM All three deletions are restricted to a region between TACSTD1 ex7 and the MSH2P4 fluorescent fragments. Thus they do not extend into the promoter of MSH2.
Long Range PCR • Used to confirm and estimate the size of the deletions in these families. • Fermentas long range PCR kit used. • Used approximately 50ngµl-1
Long range PCR: agarose gel Standard curve using λ DNA ladder λ KB 23.1 NC SR NM EM -VE 9.4 6.6 2.3 Deletions: Patient SR - ~5-6Kb Patients NM and EM - ~1.3Kb 2
Conclusion • Does the deletion detected by MLPA extend into the promoter? • Is the deletion in either of these two families related to the apparent loss of MSH2 by IHC and MSI+ phenotype? • What is the clinical significance of a deletion in the TACSTD1 gene?
TACSTD1 (A.K.A. EpCAM) Will deletions of EpCAM influence the prognosis of a patient?