Download
1 / 1
10 likes | 121 Views
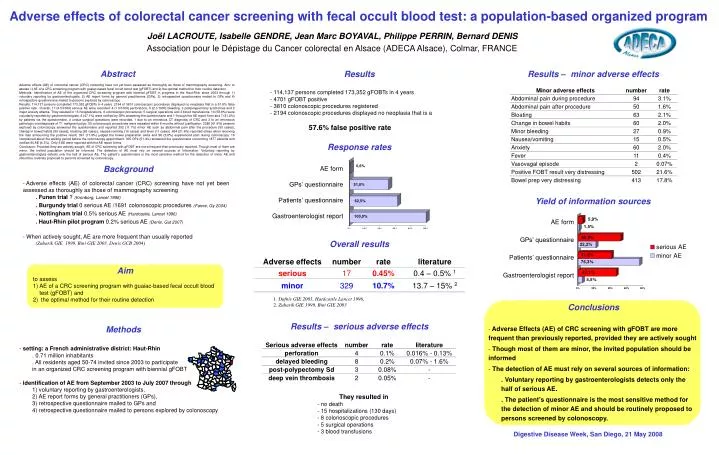
Adverse effects of colorectal cancer screening with fecal occult blood test: a population-based organized program. Joël LACROUTE, Isabelle GENDRE, Jean Marc BOYAVAL, Philippe PERRIN, Bernard DENIS. Association pour le Dépistage du Cancer colorectal en Alsace (ADECA Alsace), Colmar, FRANCE.

E N D
Adverse effects of colorectal cancer screening with fecal occult blood test: a population-based organized program Joël LACROUTE, Isabelle GENDRE, Jean Marc BOYAVAL, Philippe PERRIN, Bernard DENIS Association pour le Dépistage du Cancer colorectal en Alsace (ADECA Alsace), Colmar, FRANCE Abstract Results Results – minor adverse effects Adverse effects (AE) of colorectal cancer (CRC) screening have not yet been assessed as thoroughly as those of mammography screening. Aim: to assess 1) AE of a CRC screening program with guaiac-based fecal occult blood test (gFOBT) and 2) the optimal method for their routine detection. Methods: Identification of AE of the organized CRC screening program with biennial gFOBT in progress in the Haut-Rhin since 2003 through 1) voluntary reporting by gastroenterologists, 2) AE report forms by general practitioners (GPs), 3) retrospective questionnaire mailed to GPs and 4) retrospective questionnaire mailed to persons explored by colonoscopy. Results: 114,137 persons completed 173,352 gFOBTs in 4 years. 2194 of 3810 colonoscopic procedures displayed no neoplasia that is a 57.6% false positive rate. Overall, 17 (4.5/1000) serious AE were recorded: 4 (1.0/1000) perforations, 8 (2.1/1000) bleeding, 3 postpolypectomy syndromes and 2 major anxiety attacks. They resulted in 15 hospitalizations, 6 colonoscopic procedures, 5 surgical operations and 3 blood transfusions. 10 (58.8%) were voluntarily reported by gastroenterologists, 8 (47.1%) were notified by GPs answering the questionnaire and 1 through the AE report form and 7 (41.2%) by patients via the questionnaire. 4 undue surgical operations were recorded, 1 due to an erroneous CT diagnosis of CRC and 3 to an erroneous pathologic overdiagnosis of T1 malignant polyp. 50 colonoscopic procedures were repeated within 6 months without justification. 2288 (61.6%) persons explored by colonoscopy answered the questionnaire and reported 252 (11.1%) minor AE such as abdominal pain after the procedure (50 cases), change in bowel habits (59 cases), bloating (62 cases), nausea/vomiting (16 cases) and fever (11 cases). 494 (21.6%) reported stress when receiving the mail announcing the positive result, 397 (17.4%) judged the bowel preparation awful and 86 (3.8%) experienced pain during colonoscopy. 16 complained about the waiting period before the colonoscopy appointment. 305 GPs (51.4%) answered the questionnaire concerning 1877 patients and notified 80 AE (4.3%). Only 6 AE were reported with the AE report forms. Conclusion: Provided they are actively sought, AE of CRC screening with gFOBT are more frequent than previously reported. Though most of them are minor, the invited population should be informed. The detection of AE must rely on several sources of information. Voluntary reporting by gastroenterologists detects only the half of serious AE. The patient's questionnaire is the most sensitive method for the detection of minor AE and should be routinely proposed to persons screened by colonoscopy. • 114,137 persons completed 173,352 gFOBTs in 4 years • 4701 gFOBT positive • 3810 colonoscopic procedures registered • 2194 colonoscopic procedures displayed no neoplasia that is a • 57.6% false positive rate Response rates AE form GPs’ questionnaire Patients’ questionnaire Gastroenterologist report Background • Adverse effects (AE) of colorectal cancer (CRC) screening have not yet been assessed as thoroughly as those of mammography screening • . Funen trial ? (Kronborg, Lancet 1996) . Burgundy trial 0 serious AE /1691 colonoscopic procedures (Faivre, Gy 2004) . Nottingham trial 0.5% serious AE (Hardcastle, Lancet 1996) . Haut-Rhin pilot program 0.2% serious AE (Denis, Gut 2007) • When actively sought, AE are more frequent than usually reported • (Zubarik GIE 1999, Bini GIE 2003, Denis GCB 2004) Yield of information sources AE form GPs’ questionnaire Patients’ questionnaire Gastroenterologist report Overall results • Aim • to assess • AE of a CRC screening program with guaiac-based fecal occult blood test (gFOBT) and • the optimal method for their routine detection 1. Dafnis GIE 2001,Hardcastle Lancet 1996, 2. Zubarik GIE 1999, Bini GIE 2003 • Conclusions • Adverse Effects (AE) of CRC screening with gFOBT are more frequent than previously reported, provided they are actively sought • Though most of them are minor, the invited population should be informed • The detection of AE must rely on several sources of information: • . Voluntary reporting by gastroenterologists detects only the half of serious AE. • . The patient's questionnaire is the most sensitive method for the detection of minor AE and should be routinely proposed to persons screened by colonoscopy. Results – serious adverse effects Methods • setting: a French administrative district: Haut-Rhin • . 0.71 million inhabitants • . All residents aged 50-74 invited since 2003 to participate • in an organized CRC screening program with biennial gFOBT • identification of AE from September 2003 to July 2007 through • 1) voluntary reporting by gastroenterologists, • 2) AE report forms by general practitioners (GPs), • 3) retrospective questionnaire mailed to GPs and • 4) retrospective questionnaire mailed to persons explored by colonoscopy • They resulted in • no death • 15 hospitalizations (130 days) • 8 colonoscopic procedures • 5 surgical operations • 3 blood transfusions Digestive Disease Week, San Diego, 21 May 2008