Download
1 / 50
500 likes | 657 Views
BASICS OF HIV TESTING: HIV testing in a time-limited setting. - Aleasha Hacault STI/HIV outreach RN - Ida-Lynn Gregan MD, CCFP. N=125. Objectives. Review current HIV testing recommendations, including HIV “indicator” conditions that should trigger testing

E N D
BASICS OF HIV TESTING:HIV testing in a time-limited setting - AleashaHacault STI/HIV outreach RN - Ida-Lynn Gregan MD, CCFP
Objectives • Review current HIV testing recommendations, including HIV “indicator” conditions that should trigger testing • Perform a basic HIV risk assessment • Confidently offer HIV testing (obtaining consent and offer the variety of testing available) • Deliver an HIV +ve test result • Perform an initial assessment on a newly diagnosed HIV+ve individual
A. HIV RISK ASSESSMENT Case Study • 47 year old female (“Susan”) • Aboriginal • Recently divorced • Dating for last 6 months • Sexually active • c/o notable change in vaginal discharge & experiencing dysuria
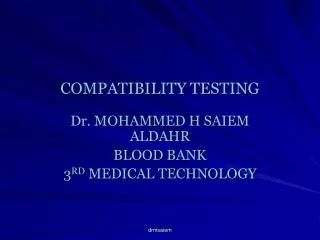
Demographic analysis new patients to care Manitoba HIV program, 2008-2010 35% 35% 35% *Risk Factors - Multiple responses; totals add up >100%
Undiagnosed HIVneed to test to diagnose! • 26% HIV+ in Canada are unaware • Undiagnosed estimated to contribute to >50 % of new HIV infections. • Being aware of HIV status reduces risk behavior in majority of HIV+ • Missed benefit of treatment on decreased transmission
Benefits of early HIV diagnosis • Benefits to the infected individual – Antiretroviral therapy (ART) Reduced mortality & morbidity (near normal life expectancy) • Benefits to the public health –Reduced onward transmission - Reduction in unsafe sexual behaviour (68%) - ART-reduced infectiousness ( x 96% in HPTN 0523) – Reduced health care costs
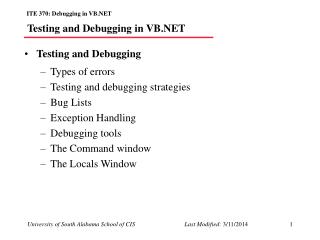
Cost-effectiveness of HIV testing (2010) Routine HIV Screening in France: Clinical Impact and Cost-Effectiveness. PLoS ONE 5(10): e13132.
US guidelinesOPT-OUT September 22, 2006 • Routine voluntary testing for patients ages 13-64 in all health care settings • Persons at high risk should be screened annually • No separate consent for HIV • Prevention counseling should not be required • Objectives • Increase screening • Foster early detection • Identify and counsel persons with unrecognized HIV infection and link them to clinical and preventative services • Reduce perinatal transmission
Test for HIV Unprotected sex (anal or vaginal w/o barrier) Sex under the influence of ETOH or drugs Tested +ve for an STI (GC, CT, Hep, syphilis) Shared needles/drug equipment Tatooing, piercing, or accupuncture (unsterile) Blood or blood products prior to Nov 1986 PHAC April 2012
Testing Only 5-10% of Manitobans (07-08) (Between Ages 15-65 yrs) Prevalence Manitoba: .3-.4% Prevalance Sasketchewan: 1%
HIDES (HIV Indicator Diseases in Europe Study) Indicator conditions: 1. AIDS-defining conditions (ADC) 2. Conditions associated with increased HIV prevalence (>0.1%) • Conditions where failure to diagnose HIV infection may have severe consequences for person’s health - Dr. Keith Radcliffe, HIV Europe March 2012, Copenhagen
AIDS-defining conditions (ADC) • Opportunistic infections – Fungal e.g. Pneumocystis jiroveci, cryptococcosis, histoplasmosis, candidiasis (oesophageal, tracheal, pulmonary) – Bacterial e.g. Tuberculosis (TB), disseminated Mycobacterium avium, recurrent pneumonia or salmonella septicaemia
AIDS-defining conditions (cont’d): • Opportunistic (cont’d): – Parasitic e.g. cerebral toxoplasmosis, cryptospridiosis, microsporidiosis – Viral e.g. CMV retinitis, PML, persistent HSV • Neoplasms – Non-Hodgkin’s lymphoma, Kaposi’s sarcoma, cervical carcinoma
Strongly recommend testing(HIV prevalence >0.1%) • Sexually transmitted infections (4.06%)1 • Lymphoma (0.29%)1 • Anal cancer/dysplasia (2.90%)1 • Cervical/anal dysplasia (0.37%)1 • Herpes zoster (2.89%)1 • Hepatitis B or C (0.36%)1 • Mononucleosis-like illness (3.85%)1 • Unexplained leucopaenia or thrombocytopaenia, >4 weeks (3.19%)1
Strongly recommend testing(HIV prevalence >0.1%), cont’d: • Seborrheic dermatitis or exanthema (2.06%)1 • Unexplained oral candidiasis (6-23%) • Invasive pneumococcal disease (2.4%) • Unexplained chronic fever (3%) • Unexplained chronic diarrhoea (10-12%) • Pregnancy (0.17%)
Consider offering testing: HIV prevalencelikely >0.1% • Primary lung cancer • Lymphocytic meningitis • Visceral leishmaniasis • Oral hairy leucoplakia • Severe or recalcitrant psoriasis • Guillain-Barré syndrome • Mononeuritis • Peripheral neuropathy • Subcortical dementia • Multiple sclerosis like disease • Unexplained weight loss • Unexplained lymphadenopathy • Unexplained renal failuire
Conditions where failure to diagnose HIV infectionmay have severe consequences: • Prior to initiating aggressive immuno-suppressive therapy – Malignancy – Transplantation – Auto-immune disease • Primary space occupying lesion of the brain
A. HIV RISK ASSESSMENT Case Study • 47 year old female (“Susan”) • Aboriginal • Recently divorced • Dating for last 6 months • Sexually active • c/o notable change in vaginal discharge & experiencing dysuria
A. HIV RISK ASSESSMENT 1. Number of partners?
A. HIV RISK ASSESSMENT 2. Type of partners/relationship? Known Unknown
A. HIV RISK ASSESSMENT 3. Use of barriers? Consistent/inconsistent use
A. HIV RISK ASSESSMENT 4. Type of sex? Vaginal Anal Oral Sex toys BDSM Non-penetrative
A. HIV RISK ASSESSMENT • Drug-use as a part of sexual experience? Drugs: legal/illegal drugs, alcohol
A. HIV RISK ASSESSMENT SUSAN’S RISK FACTORS: • Sexually active with multiple partners in past year (6 mos.) with unknown sexual histories • Vaginal, oral • High and low risk sexual activities • Known and anonymous partners • Alcohol use as part of sexual experience
PERFORMING AN HIV TEST… • Point of Care Testing (POCT, “rapid testing”) • Nominal • Non-nominal • Anonymous
PERFORMING AN HIV TEST… • POCT • Rapid results: within 60seconds to minutes • Easy and minimally invasive (finger poke) • Convenient in any setting • Accurate: >or= 99.6% specificity and sensitivity
PERFORMING AN HIV TEST… • Nominal • Test is ordered using full name of patient • Known identity of person being tested • Health Care Practitioner ordering test obligated to report positive results to Manitoba Health
PERFORMING AN HIV TEST… • Non-nominal • Test is ordered using patients initials or code • Only the person ordering the test knows the person being tested • Health care provider ordering the test is responsible for notifying Manitoba Health of positive results • Test results is linked and entered in patient’s chart
B. PERFORMING AN HIV TEST • Anonymous • Test is ordered using a bar code • Practitioner performing the test and lab do not know the identity of the person being tested • Client returns to clinic to receive results with bar code ID card
B. PERFORMING AN HIV TEST Anonymous… • If client loses card, no results can be given • Anyone can return with found card and access results • Paper copies of results are not provided
PERFORMING AN HIV TEST… Informed consent is required Verbal consent is required BUT Written consent is not required
C. OBTAINING CONSENT • Inform that you are performing test • Rationale/Indicators for test • Limitations • Consequences • Opportunity for patient to decline
CASE STUDY • Nominal testing • Indication: complete STI screen • Limitation: window period • Consequences explained • Opportunity to decline • Plan for follow-up
D. Delivering a positive result • Negative Result • Review Safer Sex Practices/Harm Reduction • Window period
D. Delivering a positive result • Positive Result • Meaning of positive result • Natural course of illness • Management & treatment • Life expectancy • Quality of life
D. Delivering a positive result • Coping • Supports • Prevention • Universal precautions • Safer sex • Issues of disclosure • Birth control • Partner notification • Public health
D. Delivering a positive result • Safety • Acute suicidality • Threats of violence to self or others
D. Delivering a positive result • Linkage to care • Manitoba HIV program: P: 940-6089; 1-866-449-0165 Fax: 940-6003 • HIV care and treatment • Counselling services • Social work; outreach • pharmacist • -Dietician • Occupational Therapy
Initial Assessment of the HIV +ve individual: • Dr. R. Barrios/ BC Centre for Excellence in HIV/AIDS: http://www.cfenet.ubc.ca/sites/default/files/uploads/Final%203-%20R.Barrios%20InitialAssessment_1.pdf
Initial assessment of the newly diagnosed HIV+ve patient: • Points to cover: • Relevant past med history • Recent hospitalizations, recurrent illnesses; past TB/exp; hepatitis • Current stressors and supports • How is pt coping with diagnosis • Any threats of violence towards pt in context of disclosure • Review ability to adhere to safer sex practices • Access to supports
Initial assessment (cont’d): • Review of systems: • Weight loss, malaise, fever, night sweats (TB, advanced HIV, lymphoma) • Eyes: change in vision (CMV retinitis) • ENT: odynophagia, dysphagia, plaques or ulcers (esophageal candidiasis, HSV esophagitis, syphilis) • Resp: cough, either productive or non; dyspnea, hemoptysis (PCP, TB, recurrent pneumonias) • Cardiac: chest pain, palp’ns
Initial assessment (cont’d): • Review of systems (cont’d): • GI: N/V, diarrhea (TB, MAC, cryptosporidiosis, advanced HIV) • GU: discharge, ulcers, warts (concurrent STIs, syphilis, HPV) • Obs/gyne: LMP (pregnancy) and pap/previous abn (cervical cancer) • Neuromuscular: peripheral numbness/tingling, or weakness (PML, CMV- associated mononeuropathy multiplex) • CNS: Headache (cryptococcal meningitis); cognitive or behavior changes (HIV-associated dementia, PML – progressvie multifocal leukoencephalopathy)
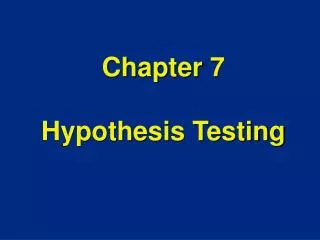
Manitoba HIV Program Structure in 2011 1050 patients: 98% in care PHARMACIST dietician Health Promotion and Outreach Education and Prevention Programs • Infectious Disease Physicians • 540 patients at hospital site • 4 nurses • Social worker • Ideal patients for this structure • Needs tertiary care services • Has a health care provider that can co-manage with us • Family doctors dedicated in HIV Care • 480 patients at Community site • 6 nurses • Social Work • Counselors • Ideal patients for this structure • Needs primary care MD in Wpg