Download
1 / 95
950 likes | 1.08k Views
Session 4: Neuromuscular Disorders. Vignette. 19 yo athlete has "tingling" in arms & legs for the 3 days with nl strength and coordination. Exam in is normal. Two days later, he is admitted with rapidly progressive weakness

E N D
Vignette • 19 yo athlete has "tingling" in arms & legs for the 3 days with nl strength and coordination. Exam in is normal. • Two days later, he is admitted with rapidly progressive weakness • Exam shows tachycardia, nl pupils, EOM, facial expression with a poor cough & gag. There is proximal weakness, areflexia and nl sensation. Bladder function is good as is rectal tone.
Questions • Which motor subsystem: muscle, neuromuscular junction, peripheral nerve, plexus, root, anterior horn cell, spinal cord, or brain is the problem located? • Differential diagnosis? • Tests • CSF findings • Management • Significance of the tachycardia and management • Prognosis • What if symptoms developed over 6 months?
Guillain-Barre Syndrome: Acute Inflammatory Demyelinating Polyneuropathy (AIDP) Georges Charles Guillain Jean-Alexandre Barre André Strohl Jean Landry
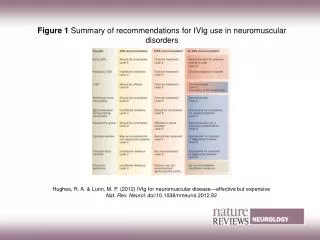
GBS • Causes: In about 80% of the patients, symptoms began about 5 days to 3 weeks after a mild infection, surgery, etc. Some have infection by Campylobacter jejuni • Treatment includes plasmapheresis (plasma exchange, PLEX) and/or high-dose immunoglobulin therapy.
Muscle NMJ Nerve ALS Cord Prox/distal P P D/P D/P D/P Sensory - - + - + Prom fascic - - + ++ - Reflexes - nc - + + EOM + + + - - Dysarth/dysph + + + + - Bladder - - + - +
??? diab neurop CIDP CMT I CMT II Axonal vs Demyelin A or D A or D Sens vs. sensmotor Both Length-dep Yes
Muscle Tone: Hypotonia/Atonia: Reduce or absent tone; associated with LMN or cerebellar lesions or acute UMN insult (e.g., spinal shock) Increased tone Rigidity Present bidirectional – associated with basal ganglia/extrapyramidal lesions (when accompanied with tremor there is “cogwheeling”). Changes in tone may be accentuated with contralateral limb activation. Performed by passively moving appendicular or axial structures Spasticity Velocity dependent; unidirectional increase in tone; associated with UMN lesion Paratonia Also known as “gegenhalten”; which is apparent increase in tone due to patient’s inability to relax; often present in individuals with cognitive changes
Function Root Nerve Deltoid Sh ab C5 Axillary Biceps flex C5/6 Musculocutan Triceps ext C6 Radial Finger ext ext C7 Radial APB abd C8/T1 Median FDI abd C8/T1 Ulnar Iliopsoas Hip flex L12 Upper plexus Quadriceps Leg ext L234 Femoral Hamstrings Leg flex S1 Sciatic Tibialis ant Dorsi L45 Peroneal Gastroc Plantar S1 Tibial EHL Dorsi L5 Peroneal
Median Nerve Musculocutaneous Nerve
Radial Nerve Ulnar Nerve
Obturator Nerve Tibial Nerve
Deep Tendon Reflexes : Adequate Relaxation Stretch Tendon Suddenly Reinforcement Grading 0 to 4
Deep Tendon Reflex Technique: Adequate Relaxation Stretch Tendon Suddenly Reinforcement Grading 0 to 4
Abnormal Plantar Response: Extension of the great toe and fanning of other toes implies upper motor neuron dysfunction. Babinski