Download
1 / 16
210 likes | 518 Views
Rheumatology: SLE. Dr. Meg- angela Christi Amores. Systemic Lupus Erythematosus (SLE). autoimmune disease in which organs and cells undergo damage mediated by tissue-binding autoantibodies and immune complexes 90% are women in childbearing years all ethnic groups are susceptible.

E N D
Rheumatology: SLE Dr. Meg-angela Christi Amores
Systemic Lupus Erythematosus (SLE) • autoimmune disease in which organs and cells undergo damage mediated by tissue-binding autoantibodies and immune complexes • 90% are women in childbearing years • all ethnic groups are susceptible
Pathogenesis • Interactions between susceptibility genes and environmental factors result in abnormal immune responses • (1) activation of innate immunity • (2) lowered activation thresholds of adaptive immunity cells • (3) ineffective regulatory and inhibitory CD4+ and CD8+ T cells • (4) reduced clearance of apoptotic cells and of immune complexes
result in abnormal immune responses • generate pathogenic autoantibodies and immune complexes that deposit in tissue, activate complement • cause inflammation • lead to irreversible organ damage
Pathogenesis • The result of these abnormalities is sustained production of pathogenic autoantibodies : • ANA (antinuclear antibodies) • Anti-dsDNA • Anti-Sm • Anti-RNP • Anti-Ro • Anti-La • Antihistone
Pathogenesis • SLE is a multigenic disease • In most genetically susceptible individuals, normal alleles of multiple normal genes each contribute a small amount to abnormal immune responses • if enough variations accumulate, disease results
Pathogenesis • Female sex is permissive for SLE • make higher antibody responses than males • Women exposed to estrogen-containing oral contraceptives or hormone replacement have an increased risk of developing SLE • environmental stimuli may influence SLE : • Exposure to ultraviolet light • some infections
Diagnosis • based on characteristic clinical features and autoantibodies • Most patients experience exacerbations interspersed with periods of relative quiescence • Antinuclear antibodies (ANA) are positive in >98% of patients during the course of disease; repeated negative tests suggest that the diagnosis is not SLE
diagnosis • Mnemonics: SOAP BRAIN MD • Serositis • Oral ulcers • Arthritis • Photosensitivity • Blood (all are low, anemia, etc) • Renal (protein, nephritis) • ANA • Immunologic (ds DNA) • Neurologic (seizures) • Malar rash • Discoid rash • > 4 out of 11 suggests SLE is highly likely
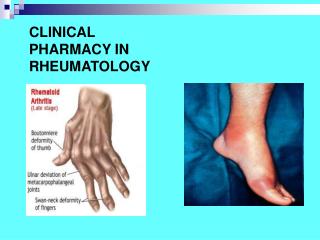
Manifestations • Arthritis – polyarthritis • soft tissue swelling and tenderness in joints, most commonly in hands, wrists, and knees • Myositis with clinical muscle weakness
Manifestations • Dermatitis • Discoid rash - roughly circular with slightly raised, scaly hyperpigmentederythematous rims and depigmented, atrophic centers • Malar rash - photosensitive, slightly raised erythema, occasionally scaly, on the face (particularly the cheeks and nose—the "butterfly" rash), ears, chin, V region of the neck, upper back, and extensor surfaces of the arms
Manifestations • Neprhritis • most serious manifestation of SLE • leading causes of mortality in the first decade of disease • Nervous system manifestations • cognitive dysfunction, including difficulties with memory and reasoning • seizures
Manifestations • Vascular occlusions • Pleuritis with or without pleural effusion • Pericarditis • Anemia, Leukopenia, Lymphopenia, Thrombocytopenia
Treatment • There is no cure • physician should plan to control acute, severe flares and then develop maintenance strategies
Treatment • Conservative strategies: (for non-life threatening cases) • suppression of symptoms • Analgesics and antimalarials • NSAIDs are useful analgesics/anti-inflammatories, particularly for arthritis/arthralgias • Antimalarials (hydroxychloroquine, chloroquine, and quinacrine) often reduce dermatitis, arthritis, and fatigue
Treatment • Life-threatening: • systemic glucocorticoids • methylprednisolone sodium succinate • Prednisone • doses are tapered as rapidly as the clinical situation permits • Cytotoxic/immunosuppressive agents added to glucocorticoids