Download
1 / 48
560 likes | 2.76k Views
Gallstones Types. Cholesterol stones Pigment stones black stones brown stones. Factors associated with black pigment stones formation. Chronic liver disease (increased frequency with severity) Ileal resection Chronic haemolysis sickle cell anaemia hereditary spherocytosis

E N D
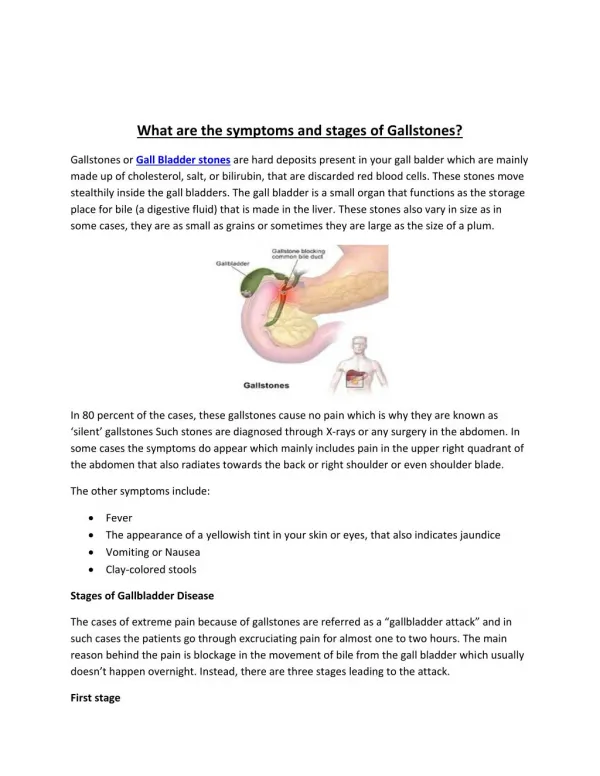
GallstonesTypes • Cholesterol stones • Pigment stones • black stones • brown stones
Factors associated with black pigment stones formation • Chronic liver disease (increased frequency with severity) • Ileal resection • Chronic haemolysis • sickle cell anaemia • hereditary spherocytosis • thalassemia major • Total parenteral nutrition • Vagotomy
Reasons for gallstone formation in cirrhosis • Cirrhotic liver unable to convert all unconjugated bilirubin into bilirubin mono- and di-glucuronides • Small fraction of unconjugated bilirubin spills into bile • Unconjugated bilirubin precipitated with calcium
Brown pigment stones formation Bilirubin diglucuronide hydrolysis by -glucuronidase Unconjugated bilirubin +Ca ion Calcium bilirubinate
Cholesterol gallstonesPathogenesis • Supersaturated bile with cholesterol due to enhanced hepatic synthesis • Low bile salt pool • Poor contractility of gallbladder • Excessive bile mucus glycoprotein
Calcified shadow at right upper abdomen in X-rayDifferential diagnosis
Cholecystectomy for asymptomatic gallstonesIndication • Calcified gallbladder • Young patients with sickle cell disease • Patients on long-term TPN
Complications of gallstonesInside the gallbladder • Acute cholecystitis • Empyema gallbladder • Mucocele of gallbladder • Carcinoma
Complications of gallstonesOutside the gallbladder • Perforation into peritoneal cavity • peritonitis or abscess • Perforation into duodenum, colon • gallstone ileus • Perforation into liver bed • liver abscess • Perforation into CBD • bile duct obstruction (Mirizzi syndrome)
Mirizzi syndrome (Cholecystocholedochal fistula)
Complications of gallstonesIn the common bile duct • Obstructive jaundice • Acute cholangitis • Acute pancreatitis
Postcholecystectomy syndrome • Persistent symptom after cholecystectomy • Due to technical complication of cholecystectomy and/or missed pathology which is the real cause of original symptom
Postcholecystectomy syndromeInvestigation • CBP, RFT, LFT, amylase • Upper endoscopy • US/CT • ERCP • HAG SMA
Acute cholangitisAetiology • Stones • Malignancy • Biliary stricture • Anastomotic stricture
To hepatic vein cholangiovenous reflux Cholangio-lymphatic reflux Venous system Stones obstructing the bile duct
Acute cholangitisAetiology • Predisposing causes • obstruction to bile duct • bacterial growth in bile
Acute cholangitis • Reynold’s pentad • Fever/chill/rigor • Right upper quadrant pain • Jaundice • Hypotension • Mental confusion
Acute cholangitisManagement - initial & conservative • Nil by mouth • IV fluid • Blood tests • Blood crossmatch • Antibiotic • Analgesic • Monitoring • BP, pulse, temperature, urine output
Acute cholangitisRationale of conservative treatment • 70% will resolve • Related to spontaneous stone disimpaction
Acute cholangitisClinical manifestation of failure of conservative treatment • temperature, pulse • BP • urine output • sensorium • abdominal tenderness, guarding
Acute cholangitisTreatment for failure of conservatism • Invasive monitoring • CVP • arterial line • pulmonary artery wedge pressure • Inotrope • Mannitol
Acute cholangitisTreatment for failure of conservatism • Biliary decompression and drainage • Surgery • choledochotomy • exploration of CBD • T-tube drainage • avoid choledochoscopy • avoid cholangiography • ± cholecystectomy
Function of T-tube after exploration of common bile duct • Serves to allow infected bile draining into the external environment and prevent elevation of intraductal pressure (and bile leakage through the suture line or holes) if there is oedema of lower end of CBD or residual CBD stones • For postoperative cholangiogram on day 7-10
Action after T-tube cholangiogram No residual CBD stone Spigot T-tube Fever + Fever - Release spigot Keep T-tube spigot for 6 weeks Re-do cholangiogram for possible CBD stone Remove T-tube
Action after T-tube cholangiogram Residual CBD stone + Keep T-tube for 2-3 months Choledochoscopy via fibrous T-tube tract
T-tube in common bile duct and residual CBD stones T-tube induces formation of fibrous tissue around it
Fibrous tract formed around T-tube serves as a conduit for choledochoscopy
Insertion of choledochoscope into the common bile duct through T-tube tract for extraction of residual CBD stones
Acute cholangitisTreatment for failure of conservatism • Biliary decompression • Endoscopy • endoscopic retrograde cholangio-pancreatography • endoscopic papillotomy • basket removal of stone • nasobiliary drainage • endoprosthesis
Acute cholangitisTreatment for failure of conservatism • Biliary decompression • Radiology percutaneous transhepatic biliary drainage (PTBD)
Percutaneous transhepatic biliary drainage (External type)
Percutaneous transhepatic biliary drainage (External-internal type)
Acute cholangitis Strategy of treatment Conservatism Failure Success Endoscopic drainage Imaging of bile duct Radiological drainage Surgery Surgical drainage