Download
1 / 1
10 likes | 173 Views
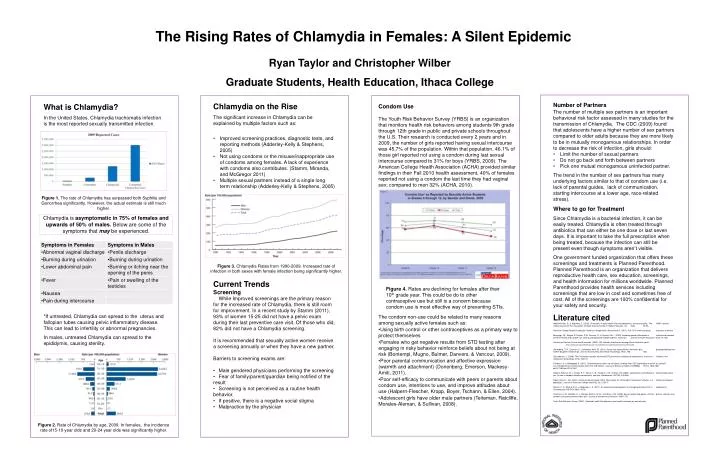
The Rising Rates of Chlamydia in Females: A Silent Epidemic. Ryan Taylor and Christopher Wilber Graduate Students, Health Education, Ithaca College. Number of Partners

E N D
The Rising Rates of Chlamydia in Females: A Silent Epidemic Ryan Taylor and Christopher Wilber Graduate Students, Health Education, Ithaca College • Number of Partners • The number of multiple sex partners is an important behavioral risk factor assessed in many studies for the transmission of Chlamydia. The CDC (2009) found that adolescents have a higher number of sex partners compared to older adults because they are more likely to be in mutually monogamous relationships. In order to decrease the risk of infection, girls should: • Limit the number of sexual partners • Do not go back and forth between partners • Pick one mutual monogamous uninfected partner. • The trend in the number of sex partners has many underlying factors similar to that of condom use (i.e. lack of parental guides, lack of communication, starting intercourse at a lower age, race-related stress). • Where to go for Treatment • Since Chlamydia is a bacterial infection, it can be easily treated. Chlamydia is often treated through antibiotics that can either be one dose or last seven days. It is important to take the full prescription when being treated, because the infection can still be present even though symptoms aren’t visible. • One government funded organization that offers these screenings and treatments is Planned Parenthood. Planned Parenthood is an organization that delivers reproductive health care, sex education, screenings, and health information for millions worldwide. Planned Parenthood provides health services including screenings that are low in cost and sometimes free of cost. All of the screenings are 100% confidential for your safety and security. • Literature cited • Adderley-Kelly, B., & Stephens, E. (2005). Chlamydia: A major health threat to adolescents and young adults. The ABNF Journal: Official Journal Of The Association Of Black Nursing Faculty In Higher Education, Inc, 16(3), 52-55. • American College Health Association, National College Health Assessment II, (2011). Fall 2011 reference group executive summary. • Bontempi, J.B., Mugno, R. Bulmer, S.M., Danvers, K., & Vancour, M.L., (2009). Exploring gender differences in relationship between HIV/STD testing and condom use among undergraduate college students. American Journal of Health Education. 40(2), 97-105. • Centers for Disease Control and Prevention. (2009). HIV-related risk behaviors among African American youth. http://www.cdc.gov/Healthyyouth/sexualbehaviors/pdf/AfricanAmericanHIV.pdf. • Donenberg, G. R., Emerson, E., & Mackesy-Amiti, M. (2011). Sexual risk among African American girls: psychopathology and mother-daughter relationships. Journal of Consulting and Clinical Psychology, 79(2), 153- 158. • Chiaradonna, C. (2008). The Chlamydia cascade: enhanced STD prevention strategies for adolescents. Journal Of Pediatric And Adolescent Gynecology, 21(5), 233-241. • Friedman, A., & Bloodgood, B. (2010). 'Something we'd rather not talk about': findings from CDC exploratory research on sexually transmitted Disease Communication with Girls and Women. Journal of Women's Health (15409996), 19(10), 1823-1831. doi:10.1089/jwh.2010.1961 • Halpern-Flescher, B. L., Kropp, R. Y., Boyer, C. B., Tschann, J. M., & Ellen, J.M. (2004). Adolescents’ self-efficacy to communicate about sex: Its role in condom attitudes commitment, and use. Adolescence. 39(155), 443-456. • Sipkin, Diane L., Alix Gillam, and Laurie Bisset Grady. 2003. Risk factors for "Chlamydia Trachomatis" infection in a california collegiate population. Journal of American College Health 52, no. 2: 65-71. • Stamm, C. A., Mirand, R. H., & Mcgregor, J. A. (2011). An evidence-based approach to managing common STIs in adolescents. Contemporary OB/GYN, 56(9), 43-50. • Teiteman, A. M., Ratcliffe, S. J., Morales-Aleman, M. M., & Sullivan, C.M. (2008). Sexual relationship power, intimate partner violence, and condom use among minority urban girls. Journal of Interpersonal Violence. 1694-1712. • Youth Risk Behavior Survey (2009). Selected health Risk behaviors and health outcomes by race/ethnicity • Chlamydia on the Rise • The significant increase in Chlamydia can be explained by multiple factors such as: • Improved screening practices, diagnostic tests, and reporting methods (Adderley-Kelly & Stephens, 2005) • Not using condoms or the misuse/inappropriate use of condoms among females. A lack of experience with condoms also contributes. (Stamm, Miranda, and McGregor 2011) • Multiple sexual partners instead of a single long term relationship (Adderley-Kelly & Stephens, 2005) • Current Trends • Screening • While Improved screenings are the primary reason for the increased rate of Chlamydia, there is still room for improvement. In a recent study by Stamm (2011), 93% of women 15-25 did not have a pelvic exam during their last preventive care visit. Of those who did, 82% did not have a Chlamydia screening. • It is recommended that sexually active women receive a screening annually or when they have a new partner. • Barriers to screening exams are: • Male gendered physicians performing the screening • Fear of family/parent/guardian being notified of the result • Screening is not perceived as a routine health behavior. • If positive, there is a negative social stigma • Malpractice by the physician • Condom Use • The Youth Risk Behavior Survey (YRBS) is an organization that monitors health risk behaviors among students 9th grade through 12th grade in public and private schools throughout the U.S. Their research is conducted every 2 years and in 2009, the number of girls reported having sexual intercourse was 45.7% of the population. Within that population, 46.1% of those girl reported not using a condom during last sexual intercourse compared to 31% for boys (YRBS, 2009). The American College Health Association (ACHA) provided similar findings in their Fall 2010 health assessment, 40% of females reported not using a condom the last time they had vaginal sex; compared to men 32% (ACHA, 2010). • The condom non-use could be related to many reasons among sexually active females such as: • Using birth control or other contraceptives as a primary way to protect themselves • Females who get negative results from STD testing after engaging in risky behavior reinforce beliefs about not being at risk (Bontempi, Mugno, Bulmer, Danvers, & Vancour, 2009). • Poor parental communication and affective expression (warmth and attachment) (Donenberg, Emerson, Mackesy-Amiti, 2011). • Poor self-efficacy to communicate with peers or parents about condom use, intentions to use, and improve attitudes about use (Halpern-Flescher, Kropp, Boyer, Tschann, & Ellen, 2004). • Adolescent girls have older male partners (Teiteman, Ratcliffe, Morales-Aleman, & Sullivan, 2008). What is Chlamydia? In the United States, Chlamydia trachomatis infection is the most reported sexually transmitted infection. *If untreated, Chlamydia can spread to the uterus and fallopian tubes causing pelvic inflammatory disease. This can lead to infertility or abnormal pregnancies. In males, untreated Chlamydia can spread to the epididymis, causing sterility. Figure 1. The rate of Chlamydia has surpassed both Syphilis and Gonorrhea significantly. However, the actual estimate is still much higher. Chlamydia is asymptomatic in 75% of females and upwards of 50% of males. Below are some of the symptoms that may be experienced. Figure 3. Chlamydia Rates from 1990-2009. Increased rate of infection in both sexes with female infection being significantly higher. Figure 4. Rates are declining for females after their 10th grade year. This could be do to other contraceptive use but still is a concern because condom use is most effective way of preventing STIs. Figure 2. Rate of Chlamydia by age, 2009. In females, the incidence rate of15-19 year olds and 20-24 year olds was significantly higher.