Download
1 / 11
130 likes | 212 Views
Learn about Primary Amoebic Meningoencephalitis (PAM) caused by Naegleria fowleri and Acanthamoeba spp., the life cycles of these amoebae, associated diseases like Granulomatous Amoebic Encephalitis (GAE) and Amebic Keratitis, symptoms, diagnosis, and treatments.

E N D
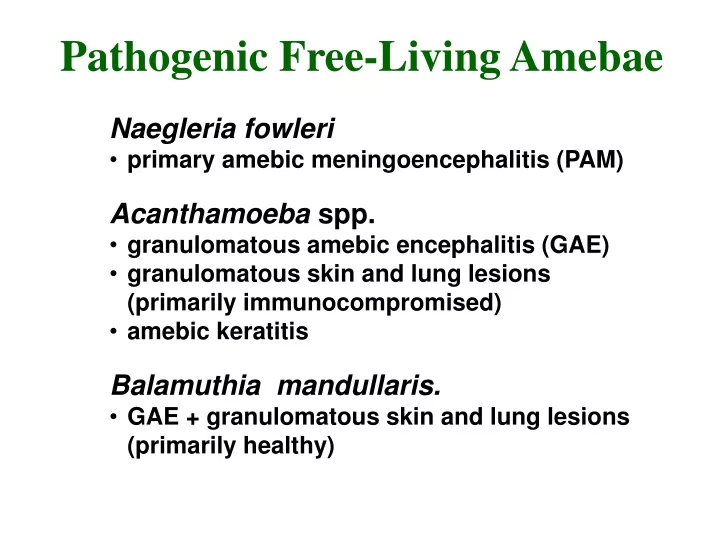
Pathogenic Free-Living Amebae • Naegleria fowleri • primary amebic meningoencephalitis (PAM) • Acanthamoeba spp. • granulomatous amebic encephalitis (GAE) • granulomatous skin and lung lesions (primarily immunocompromised) • amebic keratitis • Balamuthia mandullaris. • GAE + granulomatous skin and lung lesions (primarily healthy)
Naegleria Life Cycle low nutrients desiccation Cyst = dormant form
Naegleria fowleri • ubiquitous genus found in fresh water lakes and ponds • PAM first recognized by Fowler (1965) • initially thought to be Acanthamoeba • Naegleria fowleri is only species associated with PAM • ~ 200 documented cases worldwide • 81 in U.S. • 14 cases from same lake in Virginia • 16 cases from same stream feed pool in Czech Republic
Primary Amebic Meningoencephalitis (PAM) • 1-14 days incubation period • symptoms usually within a few days after swimming in warm still waters • infection believed to be introduced through nasal cavity and olfactory bulbs • symptoms include headache, lethargy, disorientation, coma • rapid clinical course, death in 4-5 days after onset of symptoms • trophozoites can be detected in spinal fluid, but diagnosis is usually at autopsy • 4 known survivors treated with Amphotericin B
in vitro culture brain section “lobopodia”
Acanthamoeba • ubiqutous ameba of the soil and water • Culbertson (1958) fortuitously produced disease in mice (culture contaminant) • human cases first reported in the early 70's • 73 cases worldwide of GAE as of 1991 • 39 in U.S. • majority of patients are chronically ill, immunocompromised, or debilitated with other diseases • also produces amebic keratitis and skin and lung lesions
Acanthamoeba Meningoencephalitis • portal of entry unknown, possibly respiratory tract, eyes, skin • presumed hematogenous dissemination to the CNS • infection associated with debilitation or immunosuppression • onset is insidious with headache, personality changes, slight fever • progresses to coma and death in weeks to months • amebas not yet detected in spinal fluid • trophozoites and sometimes cysts detectable in histological examination • no human cures documented
Amebic Keratitis • predisposing factors • ocular trauma • contact lens (contaminated cleaning solutions) • symptoms • ocular pain • corneal lesions (refractory to usual treatments) • diagnosis • demonstration of amebas in corneal scrapings • treatment • difficult, limited success • corneal grafts often required



![[PDF] Free Download Booted By Pam Godwin](https://cdn4.slideserve.com/8011651/slide1-dt.jpg)
![[PDF] Free Download The Diplomat's Wife By Pam Jenoff](https://cdn4.slideserve.com/8023392/slide1-dt.jpg)

![[PDF] Free Download The Lost Girls of Paris By Pam Jenoff](https://cdn4.slideserve.com/8166193/slide1-dt.jpg)