Download
1 / 126

E N D
A 55-year-old woman with a history of orthotopic lung transplantation due to pulmonary fibrosis secondary to scleroderma was on multiple medications, including Immuran, Prednisone, Prilosec, Bactrim, Lasix, Aspirin, folate, and ferrous sulfate, among others. During follow-up, she developed acute mid-abdominal pain, nausea, belching and episodes of emesis. Esophago-gastro-duodenoscopy was performed which showed acute esophagitis, gastritis and ulceration of the distal esophagus.
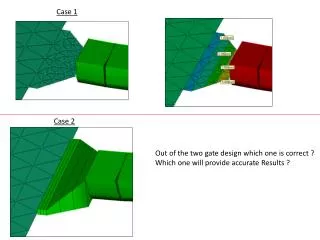
Choose the correct diagnosis: b. Gastroesophageal reflux diseasec. Thermal injury to the esophagusd. Fungal esophagitis a. Pill-associated esophagitis
The diagnosis is pill-associated esophagitis, most probably secondary to ferrous sulfate. The esophageal mucosa shows a tan-brown discoloration and encrustration of the squamous cells with a refractile light brown pigment that neatly outlines and encases the squamous epithelial cells. A minor degree of acute esophagitis is also present. There is no evidence of necrosis of the superficial cells in a laminar pattern. A brightly positive Prussian blue reaction indicates the brown pigment to be iron.
Medication-associated injury to the esophageal mucosa is usually a consequence of swallowing pills at bedtime without sufficient fluid to wash them down. This is particularly prone to occur in elderly patients and those who are somewhat obtunded. Prolonged contact of the pill or medication seems to facilitate the local injury. Ferrous sulfate is among the medications known to cause esophagitis. Some of the more common medications associated with esophagitis are tetracycline, quinidine, corticosteroids, NSAIDs, oral contraceptives, alendronate, and antibiotics.
Typically the injury is localized and produces an ulcer in the mid or distal esophagus. The diagnosis is made with a careful history and clinico-pathological correlation, although in this case the medication itself serves as a diagnostic marker of the injurious agent. The epithelial cellular encrustation and crystalline nature of the pigment seen in this case is most likely of exogenous origin (iron pill) and the likely cause of esophageal injury.
A 34-year-old male patient with a history of gastroesophageal reflux disease was incidentally found to have a 1x0.5 cm broad-based, smooth nodule at 37 cm from the incisors during esophagoscopy. The nodule was endoscopically resected.
Choose the correct diagnosis: a. Squamous cell carcinoma b. Spindle cell type squamous carcinoma c. Gastrointestinal stromal tumor (GIST) d. Leiomyoma e. Granular cell tumor
The diagnosis in this case is granular cell tumor, with pseudo-epitheliomatous hyperplasia. The plump spindled and epitheloid tumor cells have an eosinophilic granular cytoplasm and are filled with coarse red granules and occasional large globules. The tumor cells are arranged in broad fasicles and occasionally in small nests. The tumor involves the superficial lamina propria of the esophagus, where the overlying epithelium shows proliferation. The proliferating squamous epithelial nests interdigitate with the underlying connective tissue of the lamina propria as well as the granular cell tumor. The squamous epithelium is mature, showing narrow bands of downward growth, as well as disjointed islands of squamous epithelium with intercellular bridges and no evidence of cellular atypia.
Pseudo-epitheliomatous hyperplasia is often observed overlying granular cell tumors. A misdiagnosis of squamous cell carcinoma is a classic pitfall in diagnostic surgical pathology. A superficial biopsy that contains little or no granular tumor cells is a typical trap for the unwary surgical pathologist. Once the granular cell tumor is recognized in the H&E section and confirmed by an S-100 protein or PAS stain, the benign and pseudo-epitheliomatous nature of the squamous proliferation becomes obvious. The tumor cells, which at one time were thought to be myogenic in origin are typically S-100 protein positive and are currently thought to be of schwannian derivation. In the esophagus these tumors can be single or multiple, superficial or deep-seated, and can occur anywhere along the length of the esophagus. Within the gastrointestinal tract, the esophagus appears to be a relatively common site for the occurrence of granular cell tumors
Choose the correct diagnosis: • a. Hepatocellular carcinoma • b. Metastatic adenocarcinoma • c. Metastatic carcinoid tumor • d. Cholangiocarcinoma
The tumor is composed of nests and cords of cells with uniform round to oval nuclei. The nuclear chromatin is fine and has a "salt and pepper" quality. Numerous mitotic figures can be identified within the tumor.
The tumor cells show neuroendocrine chromatin with salt and pepper nuclei. The nuclear features favor a diagnosis of a neuroendocrine tumor. However, immunohistochemical stains for neuroendocrine markers such as chromogranin and synaptophysin can be performed to confirm a neuroendocrine tumor and to rule out metastatic or primary adenocarcinoma. Although primary carcinoid tumor can occur in the liver, the majority of cases are metastatic from another primary site. In this particular case, the patient had a history of a lung carcinoid. In the absence of a clinical history, immunohistochemical stains may be helpful in identifying the source of the primary carcinoid tumor. Thyroid transcription factor-1 (TTF-1) is a nuclear protein expressed in thyroid, lung and forebrain. TTF-1 is expressed in 70 to 80% of pulmonary carcinoid tumors, and in 0 to 2% of gastrointestinal carcinoid tumors and pancreatic endocrine tumors.
A young female with right upper quadrant pain and a discrete liver lesion
Choose the correct diagnosis: • a. Focal nodular hyperplasia • b. Cirrhosis • c. Nodular regenrative hyperplasia • d. Congenital hepatic fibrosis
Histology: This lesion is characterized by bridging fibrosis and regenerative nodules of hepatocytes. There is a central scar in which abnormally structured blood vessels are present.
Discussion: The process is histologically identical to cirrhosis; however, we are told that the process is focal. Therefore, the diagnosis is "focal cirrhosis" , also known as focal nodular hyperplasia. Cirrhosis requires that the liver diffusely demonstrate bridging fibrosis and nodular regenerative hyperplasia of hepatocytes. Nodular regenerative hyperplasia characterized by diffuse micronodular transformation of the liver in the absence of bridging fibrosis. Congenital hepatic fibrosis is characterized by diffuse fibrosis within the liver bridging portal tracts, but regenerative nodules of hepatocytes are not found. The bile ducts have a hamartomatous appearance consistent with the hypothesis that this lesion represents a ductal malformation. Focal nodular hyperplasia is thought by many to be a reactive process in response to alteration in hepatic blood flow. The presence of dysplastic arterioles within the central scar of the lesion as seen in the current case, supports this theory.
A 54 year-old male is found to have an incidental gastric mass on imaging
Choose the correct diagnosis: • a. Schwannoma • b. Leiomyoma • c. Gastrointestinal stromal tumor (GIST) • d. Inflammatory fibroid polyp • e. Inflammatory myofibroblastic tumor
The lesion is a well-circumscribed, non-infiltrative spindle cell tumor centered in the gastric sub-serosa. Focal lymphoid aggregates are seen at the periphery of the lesion. The individual spindle cells have elongated nuclei with blunt to pointed ends and occasional perinuclear vacuoles. The nuclei are focally palisaded. There is no necrosis and no mitotic figures. Immunohistochemical stains show the lesional cells to be positive for c-kit (CD117), CD34, and DOG-1, but negative for the S100-protein.
Gastrointestinal stromal tumors (GISTs) are mesenchymal tumors that arise from the interstitial cells of Cajal, or their derivatives, which are driven primarily by KIT and to a lesser degree PDGFRA mutations. The presence of mutations in KIT is pertinent, because it enables GISTs to be treated with targeted tyrosine kinase inhibitors, such as imatinibmesylate (Gleevec). Most KIT mutations occur in exon 11, while a subset occur in exon 9; this is also pertinent, because the tumors with exon 9 mutations do not respond as well to the tyrosine kinase inhibitors. GISTs can arise anywhere along the GI tract, either sporadically or syndromically. Syndromic GISTs are associated with neurofibromatosis type 1, which is characterized predominantly by multiple neurofibromas (solitary or plexiform) café-au-lait skin pigmentation, pigmented iris hamartomas (Lisch nodules), and an increased incidence of MPNST and other soft tissue tumors. Familial GISTs also arise in the setting of hereditary KIT/PDGFRA mutations, loss of succinate dehydrogenase subunit B (SDHB), Carney triad, and Carney-Stratakis syndrome. The prognostication of GISTs depends upon the tumor site, size and mitotic rate. In general, gastric GISTs do well even with large size or moderate mitotic rate, while small intestinal (particularly jejunal/ileal) and rectal GISTs do worse.