Download
1 / 21
210 likes | 521 Views
Ali T. Taher, MD Professor Department of Internal Medicine American University of Beirut Medical Center Beirut, Lebanon. Clinical Case: Managing Iron Overload in a Patient with Transfusion-Independent Thalassaemia Intermedia. Patient Presentation.

E N D
Ali T. Taher, MD ProfessorDepartment of Internal MedicineAmerican University of Beirut Medical CenterBeirut, Lebanon Clinical Case: Managing Iron Overload in aPatient with Transfusion-Independent Thalassaemia Intermedia
Patient Presentation • 26-year-old fisherman of Mediterranean origin • Diagnosed with thalassaemia intermedia at age 3 years • Chief symptoms were pallor, mild anaemia, and mild splenomegaly • Transfused once during childhood, before splenectomy • Referred for evaluation of iron overload • Physical exam nonrevealing • Haemoglobin level 9.6 g/dL • Steady-state serum ferritin level 520 ng/mL
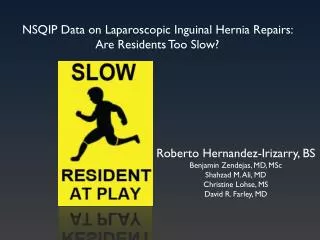
Serum Ferritin vs LIC Measurement by R2 MRI in Patients with TI TI 10,000 Linear TI 9000 TM 8000 Linear TM 7000 6000 Serum Ferritin Level (ng/mL) 5000 4000 3000 2000 1000 0 0 5 10 15 20 25 30 35 40 45 50 LIC (mg Fe/g dry weight) LIC correlated with serum ferritin levels in patients with TI (R = 0.64; P <.001) Abbreviations: LIC, liver iron concentration; TI, thalassaemia intermedia; TM, thalassaemia major.With permission from Taher A, et al. Haematologica. 2008;93:1584-1586.
Extrapolating from the above table: when LIC = 7 mg Fe/g dry wt→ serum ferritin is 604 μg/L in patients with TI LICs in patients with TM were not significantly different from values in patients with TI, whereas serum ferritin levels were statistically different between TI and TM LIC Measurement by R2 MRI in TI vs TM LIC Calculated from the Equations of the Plots of LIC vs Serum Ferritin Taher A, et al. Haematologica. 2008;93:1584-1586.
Case Continues • Patient’s liver iron concentration on R2 MRI was 11 mg Fe/g dry weight • Patient also underwent MRI T2* of the heart to evaluate for cardiac iron overload • Cardiac T2* = 36 ms (normal >20 ms)
Iron Overload and Desferrioxamine Chelation Therapy in Thalassaemia Intermedia • 6-month trial of 12-hour infusion of desferrioxamine in 10 transfusion-independent thalassaemia intermedia patients • To determine optimal dosage for iron elimination, 5 regimens were administered each day for 3 consecutive days • 20, 40, 60, 80, and 100 mg/kg/day • Maximum dose not exceeding 2 g/day • Significant lowering of serum ferritin after 6 months, with tolerable safety profile Cossu P, et al. Eur J Pediatr. 1981;137:267-271.
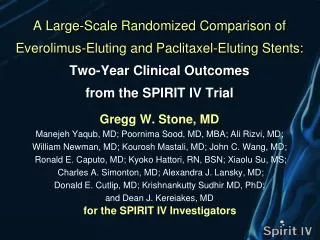
Urinary Iron Excretion by Dose of Desferrioxamine and Age of Patients with Thalassaemia Intermedia 20 mg/kg (r = .81) 60 mg/kg 40 mg/kg (r = .79) 60 mg/kg (r = .82) 10 40 mg/kg Urinary Iron (mg/24h) 5 20 mg/kg 0 0 5 10 15 Age (Years) • Significant urinary iron excretion (UIE) after 12 hours of continuous desferrioxamine (except in patients aged <1 year) • In some patients, substantial UIE despite modest serum ferritin levels • Serum ferritin levels of no value in predicting UIE With permission from Cossu P, et al. Eur J Pediatr. 1981;137:267-271.
Case Continues • After 6 months of desferrioxamine therapy the patient was re-evaluated using liver R2 MRI • LIC = 10.5 mg Fe/g dry weight • Patient’s wife admitted he was skipping most of his doses because the idea of carrying a pump around at his age created major discomfort
Reduction in Iron Burden with Deferasirox at Year 1 in Patients with TI • Mean cardiac T2* and LVEF (both normal at baseline), serum creatinine, and cystatin C did not significantly change after 12 months of treatment with deferasirox Deferasirox can effectively reduce iron burden in patients with TI Abbreviations: LVEF, left ventricular ejection fraction; TI, thalassaemia intermedia. With permission from Voskaridou E, et al. Haematologica. 2009;94(suppl 2):79(abstr 0204).
Deferasirox for Nontransfusional Iron Overload in Patients with Thalassaemia Intermedia • 11 patients with thalassaemia intermedia • 6 male, 5 female • Mean age 31.7 years • 10 splenectomized • Deferasirox regimen • 1 year (n = 11), 2 years (n = 4) • 10 mg/kg/day (n = 7), 20 mg/kg/day (n = 4) • Dose adjustment after first year Ladis V, et al. Haematologica. 2009;94(suppl 2):509(abstr 1279).
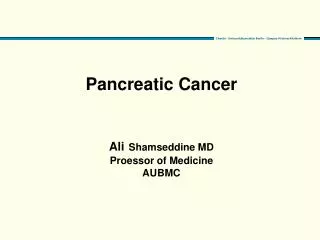
1 patient, who was noncompliant, did not show decrease of iron overload and was excluded from graph Changes in LIC and ferritin levels were related to deferasirox dose, but even patients with severe iron load, treated with 10 mg/kg/day, responded well 3000 Serum ferritin at baseline Serum ferritin at 1 year Serum ferritin at 2 years LIC at baseline LIC at 1 year LIC at 2 years 2000 Serum Ferritin Levels (ng/mL) 1000 0 Patients Effect of Deferasirox on Serum Ferritin and LIC in Patients with TI and Nontransfusional Iron Overload 40 30 LIC (mg Fe/g dry weight) 20 10 0 Patients With permission from Ladis V, et al. Haematologica. 2009;94(suppl 2):509(abstr 1279).
Safety of Deferasirox During Treatment of up to 2 Years Treatment was well tolerated No serious adverse events were noted Creatinine and cystatin C levels did not change during treatment Transaminase levels significantly decreased in year 1 (P = .0002) and year 2 (P = .024) of treatment This improvement probably due to decreased hepatic siderosis Ladis V, et al. Haematologica. 2009;94(suppl 2):509(abstr 1279).
Ongoing Clinical Evaluation of Deferasirox • Prospective, randomized, double-blind, placebo-controlled triala • Patients (age ≥10 years) with non–transfusion-dependent β-thalassaemia (no transfusion required within 6 months prior to the study) • 2 doses: 5 mg/kg/day and 10 mg/kg/day • Screening 4 weeks; treatment period 52 weeks • Primary objective • To assess the efficacy of deferasirox in patients with non–transfusion-dependent β-thalassaemia, based on the change in LIC from baseline after 1 year of treatment compared with placebo-treated patients aAli T. Taher, MD, principal investigator; Study ID ICL670A2209.
Case Continues • Patient was shifted to deferasirox 20 mg/kg/day • Over the next 2 years his liver R2 MRI measurements improved • Year 1 LIC = 5.3 mg Fe/g dry weight • Year 2 LIC = 2.9 mg Fe/g dry weight
Conclusions • Iron overload occurs in patients with thalassaemia intermedia in the absence of blood transfusions • Serum ferritin underestimates the severity of iron overload in patients with thalassaemia intermedia • Hence, the use of R2 MRI to measure LIC is favored • Initial results of the oral iron chelator deferasirox indicate that it can effectively and safely reduce iron burden in this patient population