Download
1 / 50
500 likes | 507 Views
Learn about the burden of HIV and HCV among older adults, updated testing recommendations, and strategies for open discussions with clients.

E N D
What Aging Service Providers Need to Know about HIV and HCV (Hepatitis C Virus)February 2015
Please call West DeLeon at:212-924 -3934 x134or email:wdeleon@acria.org Technical Support
Greg Olsen, Executive Mark Milano Deputy Director, NYS HIV Educator Office for the Aging ACRIA Presenters
Describe the burden of HIV and HCV among older adults. • Review updated 2014 HIV and HCV testing recommendations for older adults, and public health laws that require providers to offer HIV and HCV testing to older clients. • Explain the meaning of HIV and HCV test results in a manner older clients can understand. Training Objectives
Discuss the improvements and importance of new HCV treatment protocols and regimens. • List the benefits of educating and linking newly diagnosed HIV and/or HCV clients to care and treatment. • Identify strategies that providers can use to have open discussions with clients about HIV and HCV. Objectives (cont.)
New Cases of HIV • 1993: over 14,000 • 2013: approx. 3,000 . • Deaths from AIDS • 1994: approx. 10,000 • 2013: under 2,000 • New infections among injection drug users down 96% • New infections over the last decade down 40% • 2013: only 2 infants infected – transmission rate of 0.5% NYS Accomplishments
Reduce the number of new HIV infections per year to less than 750 by 2020 Decrease the overall number of people living with HIV for the first time NYS Plan to End AIDS
To identify people with HIV who remain undiagnosed and link them to health care To retain patients diagnosed with HIV in health care and provide access to treatment to suppress the virus, promote positive health outcomes, and prevent further transmission To provide access to PrEP for high-risk persons to keep them HIV negative Three Pillars of the Plan
2014 HIV Testing Law Update • HIV testing must be offered to all persons aged 13 – 64 as part of routine health care. • Streamlined oral consent for all HIV tests • Except in corrections • Inform patient • Document in patient chart • People must be provided key points about HIV prior to testing.
Hospital inpatient departments Emergency departments Primary care services in hospital outpatient departments Primary care services in diagnostic and treatment centers (includes school-based clinics and family planning sites) Required Offer – Where?
Physicians, physician assistants, nurse practitioners, or midwives providing primary care regardless of setting • “Primary Care” refers to: • family medicine • general pediatrics • primary care • internal medicine • primary care obstetrics/gynecology Required Offer – Which Providers?
Prior to asking for consent, providers must give key points of information about HIV. Key points may be given orally, by video, or in a written document. Individuals must be allowed to decline HIV testing Testing will only be donewith patient consent after key points are given. Before the HIV Test
HIV post-test messages must be tailored to status • Post-test information for negative results does not have to be provided face-to-face • negative result and information may be provided by mail, electronic messaging or telephone as long as patient confidentiality is reasonably protected Post-test Information
Describe meaning of test result • Discuss possibility of HIV exposure during the window period: • 12-14 days with 4th generation HIV tests • 3-4 weeks with rapid antibody tests • Emphasize HIV risks associated with sex and needle-sharing Negative Test Result
Should be discussed with those who test HIV negative Can prevent HIV infection if started within 36 hours of exposure Continued for 28 days PEP: Post-exposure prophylaxis
Should be discussed with HIV-negative people who have ongoing high HIV risk. PrEP: Pre-exposure prophylaxis
Explain the benefits of Highly Active Anti-Retroviral Treatment (HAART) and the importance of viral suppression Notification of sexual and/or needle sharing partners, including known contacts (such as spouse) Domestic violence screening Responsibility of provider to make an appointment for follow-up medical care Confirmed Positive
January, 2014 update at hivguidelines.org • Current HIV treatments: • Very effective • Easy to take • Low side effects • Reduce transmission of HIV • Offer treatment to all regardless of CD4 count NYS Clinical Guidelines for Starting Treatment
Promote HIV testing Promote linkage and retention in care Engage with health system DSRIP activitieswww.health.ny.gov/dsrip Promote sexual health Address stigma by demonstrating openness and acceptance (posters, etc.) Role of Aging Providers
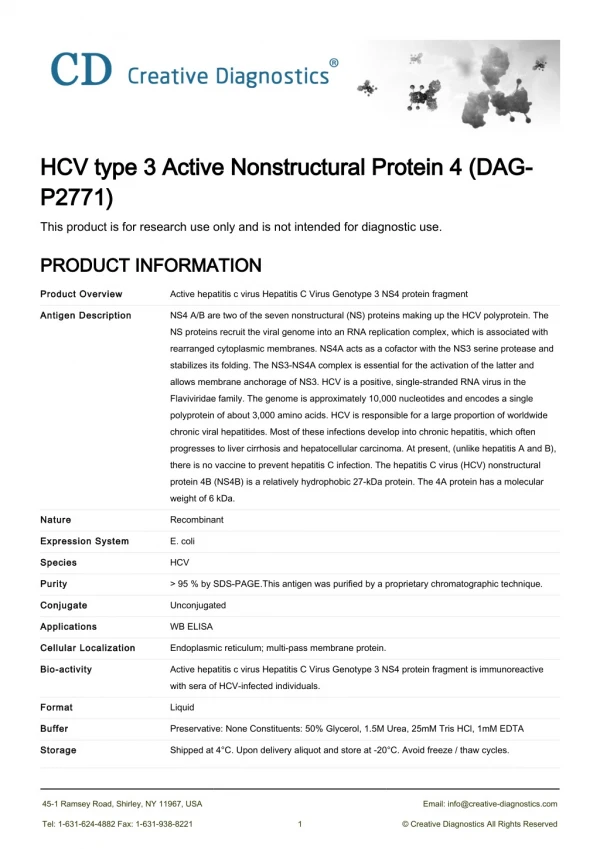
HCV Update • Transmitted through exposure to blood • Injection drug use (IDU) • Not efficiently spread through sex • More cases seen through anal sex • No vaccine • Effective treatments • HCV is curable
17,000 new infections in 2010 • Major cause of liver disease • Leading indication for liver transplants • HCV-related costs • Over $5 billion annually • Estimated 2010-2019 costs: $54.2 billion Trends in HCV in the U.S.
Persons born between 1945-1965 are five times more likely to have HCV • 3.25% among 1945-1965 • 0.88% among others • 1.94 million chronically infected • 73% of all HCV-associated mortality • 58% reported two or more drinks a day • 80% lack Hepatitis A/B vaccination HCV in People Born 1945-1965
Up to 85% of adults with chronic HCV unaware • Up to 87% of high-risk populations unaware • 45% of persons ever infected with HCV report no known risk • Liver function blood testsmiss over half of HCV cases Limited Effectiveness of Risk-Based Testing Strategy
HCV in NYS Baby Boomers Data Source: NYSDOH, Bureau of Communicable Disease Control and NYCDOHMH, Bureau of Communicable Disease Control and Prevention
First in the Nation Effective January 1, 2014 One-time HCV test must be offered to people born between 1945 and 1965. Offer of testing must be culturally and linguistically appropriate. NYS Hepatitis C Testing Law
Settings and Providers Impacted Health Care Providers Physician Physician Assistant Nurse Practitioner Providing primary care regardless of setting type Health Care Settings • Inpatient of a hospital • Outpatient department of a hospital that offers primary care services • Freestanding diagnostic and treatment center Key Question: Does the setting or provider offer primary care? If yes, then the law applies.
Age-based HCV screening recommendations do not replacethe need for screening based on risk. CDC Testing Recommendations Ever injected illegal drugs Ever on dialysis Blood transfusions /organ transplants before July 1992 Clotting factor before 1987 Known exposure to HCV Living with HIV Signs or symptoms of liver disease (abnormal ALT) Children born to mothers who have HCV
Antibodies usually detectable 8 weeks after exposure • Result can be reactive or non-reactive • A reactive result is a presumptive positive and can indicate: • Current HCV infection • Past (resolved) HCV infection • False positive • If result is reactive, an HCV RNA test should be performed to diagnose current infection HCV antibody test
Explain non-reactive test, and that a negative antibody test does not protect from future infection. Discuss that if the patient was exposed in the last 6 months, repeat screening is needed in 6 months. Provide information on HCV prevention, risk, and harm reduction. Encourage healthy choices and hepatitis A and B vaccination. For people with a non-reactive HCV test:
Explain reactive test and need for RNA test to confirm. Provide basic HCV and treatment information. Discuss minimizing risk behaviors to avoid transmitting HCV and encourage notification of partners. Discuss healthy liver practices: stopping or reducing alcohol; hepatitis A and B vaccinations Encourage healthy choices and describe the importance of regular medical care. For people with a reactive HCV test:
If test is reactive, health care provider must: • offer the individual follow-up health care , or • refer the individual to a health care provider who can provide follow-up health care • Follow-up care must include an HCV RNA test. Follow-Up Care
Determines current infection status • Often referred to as PCR test • Results may be reported as: • Detected or Not Detected (Qualitative) • A viral load or undetectable (Quantitative) • Reflex testing is available HCV RNA test
Everyone with HCV should be referred to care • Early evaluation and ongoing monitoring • Treatment response decreases as liver disease progresses • Measures to protect liver from further harm • Hepatitis A and B vaccination • Decrease or eliminate alcohol consumption • Encourage weight loss for persons who have a BMI over 25 • Reduce risk of transmission Benefits of HCV Care
Dramatic improvement in treatment • Many can be cured in just a few months! • Treatment success is measured by a sustained virologic response (SVR) • Undetectable HCV viral load 3-6 months after finishing treatment HCV Treatment
HCV Treatment before 2013 • Pegasys, PEG-Intron: Weekly alfa-interferon shots • Rebetol, Copegus : Twice daily ribavirin pills • 6 to 18 months • Low SVR rates • Many side effects
HCV Treatment Now • Sovaldi • Olysio • Harvoni (combo) • Viekira Pak (combo) • Treatment for 3 months or less • SVR rates up to 100% • Few side effects • Cost is a concern
Response Rates • Poor response to interferon/ribavirin: • African American • High HCV viral load • HIV coinfection • Not a big concern with the new treatments • Even cirrhosis does not reduce response • “All the old predictors of response are gone when you have a potent two-or-three drug combination. Response rates for HIV-positive and HIV-negative people are exactly the same.”
Treatment more successful with: • Patient education • Mental health assessment and care • Substance use counseling • Case management • Treatment adherence services • Support groups Comprehensive Care
Raise awareness about impact of HCV on baby boomers Encourage clients to access HCV testing Acknowledge advances in treatment Refer to care Address stigma by demonstrating openness and acceptance (posters etc.) Role of Aging Providers
Tools available to promote law www.cdc.gov/hepatitis
NYS Hepatitis C Information Line 1-800-522-5006 • NYS HIV/AIDS Information Hotline 1-800-541-2437health.ny.gov/forms/order_forms/hepatitis_education.pdf Additional Resources
Info on HIV and NYS testing law: • health.ny.gov/diseases/aids/providers/testing • Info on HCV and NYS testing law: • health.ny.gov/hepatitis • Click on Hepatitis C Testing • Info on Hepatitis C • cdc.gov/hepatitis • aasld.com • hivandhepatitis.com • Info on Aging and HIV • acria.org Additional Resources
Training Resources Training for Support Staff Training for Clinicians www.hivtrainingny.org www.ceitraining.org
Follow up All attendees will receive an email 1 -2 days after the webinar. Follow the instructions in order to print your certificate. For more info, contact West DeLeon at: wdeleon@acria.org