Download
1 / 57
650 likes | 1.52k Views
BLOOD 2 RED BLOOD CELLS JAUNDICE ANEMIA & POLYCYTHEMIA. CONTENT. RED BLOOD CELLS (RBC) COUNT, FUNCTIONS, STRUCTURE HEMOGLOBIN ( Hb ): CHEMISTRY, REACTIONS, FUNCTIONS, CONCENTRATION ERYTHROPOIESIS, CONTROL OF ERYTHROPOIESIS DESTRUCTION OF RBC, METABOLISM OF Hb AND IRON. HEMOSIDEROSIS

E N D
CONTENT • RED BLOOD CELLS (RBC) COUNT, FUNCTIONS, STRUCTURE • HEMOGLOBIN (Hb): CHEMISTRY, REACTIONS, FUNCTIONS, CONCENTRATION • ERYTHROPOIESIS, CONTROL OF ERYTHROPOIESIS • DESTRUCTION OF RBC, METABOLISM OF Hb AND IRON. HEMOSIDEROSIS • JAUNDICE • ERYTHROCYTE SEDIMENTATION RATE • TYPES OF ANEMIA, SICKLE CELL DISEASE • POLYCYTHEMIA
OBJECTIVES • Describe the functional consequence of the lack of a nucleus, ribosomes, and mitochondria for a) protein synthesis and b) energy production within the red blood cell. • Relate the three red blood cell concentration estimates, red blood cell count, hematocrit, and hemoglobin concentration. • Know the importance of MCV and be able to calculate the mean corpuscular volume. • Describe the structure of hemoglobin (Hb). Describe the differences between the major normal types of Hb (adult A and A2, glucosilated, fetal). Predict the changes in Hb types present in blood when synthesis of beta chains of globin is deficient. Describe the abnormal types of Hb (Hb S, thalassemias). Describe the normal and abnormal Hb reactions (oxyHb, MetHb, carboxyHb). Calculatethe mean corpuscular Hb concentration and the mean corpuscular Hb. • Identify the site of erythropoietin production, the adequate stimulus for erythropoietin release, and the target tissue for erythropoietin action. Describe the role of vitamin B12 & folic acid, and various hormones in regulation of RBC formation. Describe the dietary requirements for RBC production. Relate the rate of red blood cell production and the percentage of immature reticulocytes in the blood. • Describe the metabolism of iron in the body. • Describe the metabolism of Hb (pre-hepatic, hepatic, post-hepatic). • Describe the three types of jaundice (pre-hepatic, hepatic and post-hepatic). Compare and contrast the laboratory findings and urine/stool color in the three types of jaundice. • Describe physiological jaundice of the newborn. • Discuss the normal balance of red blood cell synthesis and destruction, including how imbalances in each lead to anemia or polycythemia.Compare and contrast the main types of anemia (nutritional, hemolytic, aplastic, hemorrhagic). Be able to describe different types of anemia in terms of MCV and MCHC.Describe the main effects of anemia and polycythemia on body functions.
RBC: Functions • Transport of O2 from the lungs to the tissues and CO2 in the opposite direction • Hemoglobin • Carbonic anhydrase • Catalyses the reaction H2O + CO2 ↔ H2CO3 • Maintenance of pH homeostasis (globin, phosphate and bicarbonate buffers)-hemoglobin in the cells is an excellent acid-base buffer • Contribution to the blood viscosity • ↓ blood oncotic P (by keeping Hb-protein inside the cells)
RBC COUNT • Normal values • Adult males: 4 600 000 – 6 200 000/mm3 (5.4million/mL) • Adult females: 4 200 000 – 5 400 000/mm3 (4.8million/mL) • Abnormally high count – polycythemia • Abnormally low count – anemia
STRUCTURE OF THE MATURE RBC Small size Excess of the plasma membrane & specific shape RBC - biconcave discs with central depression on each side High surface-to-volume ratio Deformation of the cells without stretching the plasma membrane Rapid diffusion of respiratory gases to and from the cell Easy passage through the small capillaries
Red Blood Cells Figure 16-5
STRUCTURE OF THE MATURE RBC (cont.) • Membrane contains special proteins and polysaccharides that differ from person to person – blood groups • Lack of the nucleus and organelles • Cannot undergo mitosis • Generate ATP anaerobically → do not use oxygen they transport • Can not synthesize new cellular components to replace damaged ones Life span - 120 days • Contain a red pigment, hemoglobin(red color of the blood) • Occupies 1/3 of cellular volume • 280 million Hb molecules/RBC
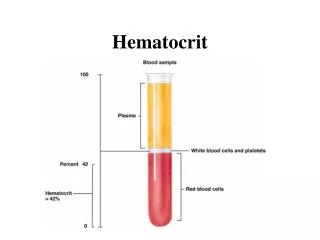
MEAN CORPUSCULAR VOLUME MCV: 82-99 fL • Mean volume of a RBC • Values • Normal range 82 – 99 femtolitre (fL) • Low volume in microcytic anemia • High volume in macrocytic anemia • Calculation of the MCV Hematocrit x 10 RBC count (in millions/mL blood) • Sample calculation: Htc = 40, RBC count = 5 (x 106/mL) MCV = (40 x 10)/5 = 80 fl fL= 10-15 L
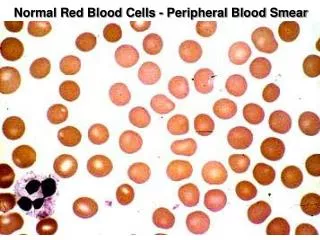
RBC Morphology In a normal individual RBCs show minimal anisocytosis(Excessive variation in the size of cells )and poikilocytosis(irregularly shaped erythrocytes). Larger than average RBCs are macrocytic (left), while those smaller than average are microcytic (right).
Pale cells (central pallor >1/3 dia) are referred to as hypochromic (right), while cells without central pallor are called hyperchromic (left). Normal peripheral blood RBCs are normochromicnormocytic.
HEMOGLOBIN: Chemistry Adult Hb – HbA, Hbα2β2 • Protein – globin • 4 polypeptide chains • Normal adult Hb – HbA,Hbα2β2 • A pair of α chains (141 AA) • A pair of β chains (146 AA) • Adult Hb –HbA2 (2.5% of Hb), Hbα2δ2 • β chains are replaced by δ chains • Fetal Hb – HbF, Hbα2γ2 • β chains are replaced by γ chains (146 AA) • Adult Hbglucosilated – HbAIc • Has a glucose attached to each β chain • Nonprotein pigment bound to each of the 4 chains – hem • Each hem ring has 1 iron ion (Fe2+) that can combine reversibly to 1 O2 molecule • Each Hb molecule can bind 4 O2 molecules
Inherited disease High prevalence in the malaria belt Mutation causes formation of HbS instead of HbA HbS precipitates into long crystals when oxygen tension is low (hypoxia) → cell elongation (sickling) and damage to the cell membrane → hemolysis → hypoxia (vicious cycle) Rigid sickled RBCs occlude the microvasculature leading to vaso-occlusive crisis. SICKLE CELL DISEASE HbS – HbαA2βS2 Negatively charged glutamate is substituted for nonpolar valine at position 6 in the β chain)
HEMOGLOBIN: Reactions • Oxyhemoglobin:Hb + 4 O2 (O2 attaches to Fe2+ in hem) • Is produced in the lungs (oxygen loading) • Reduced Hb (deoxyHb) • Is produced in tissue capillaries after dissociation of O2 (oxygen unloading) • Combines with H+ - acts as a buffer • Combines with CO2 → Carbaminohemoglobin:Hb + CO2 (CO2 binds to globin, not to hem) OxyHb O2 carrying function CO2 carrying function Buffering function COOH/COO- NH-COO- NH2/NH3+
HEMOGLOBIN: Reactions (cont.) • Methemoglobin (MetHb): • Hb iron is oxidized from the ferrous (Fe2+) to the ferric state (Fe3+) • Is incapable of carrying O2 and has a bluish color → cyanosis • Limited amount of metHb can be converted back to Hb by methemoglobinreductase present in the RBCs • In normal state, 1.5% of Hb is in MetHb state • Methemoglobinemia: Met-Hb> 1.5% (results from oxidation by nitrates, drugs like phenacetinor sulfonamides and congenital deficiency of methemoglobinreductase). • Carboxyhemoglobin:Hb + CO(carbon monoxide)→ cherry-red color of the skin and mucous membranes • CO has 200-250 times the affinity to Hb as does O2 → HbCO is a very stable molecule • CO ↓ the functional Hb concentration • HbCO is unavailable for O2 transport → CO poisoning, acute onset anemia
HEMOGLOBIN: Concentrations Concentration per unit volume of whole blood Mean corpuscular Hb concentration - concentration of Hb per unit packed cell volume MCHC = Hbamount / Volume of packed RBC Hb concentration = Hb amount (g)/Volume of whole blood (dL, L) Plasma Calculation: MCHC = Hb concentration x 100 Htc Sample calculation: [Hb] = 14.5 g/dL, Htc = 45 mL/dL MCHC = (14.5/45) x 100 = 32.2 g/dL packed cells Males – 16.0±2.0 g/dL Females – 14.0±2.0 g/dL RBC Normal range: 31-37 g/dL packed cells ↓ value – hypochromia(i.e., Hb deficiency) ↑ value – hyperchromia(i.e., spherocytosis)
Hb CONCENTRATION: Mean corpuscular Hb (MCH) • Is the total Hb content of a RBC • Values • Normal range – 27-31 pg • ↓ value – hypochromia (i.e., iron deficiency anemia) • ↑ value – hyperchromia (i.e., vit B12 deficiency) • Calculation MCH = Hbin grams/100 mL blood x 10 RBC count in million/L blood • Sample calculation: [Hb] = 12 g/dL, RBC count = 4 x 106/mL MCH = 12/4 x 10 = 30 pg MCH
Erythropoiesis • Concept: The production of new red blood cells to replace the old and died ones • In the adult, all the red cells are produced in bone marrow
Erythropoiesis- Pluripotent stem cells • in the bone marrow • can produce any type of blood cells. • is capable of both self-replication and differentiation to committed precursor cells that can produce only a specific cell line. CFU:colony-forming unit
Early Intermediate Late Proerythroblast (Pronormoblast) Polychromatophilic Normoblast Reticulocyte Basophilic Normoblast Orthochromatophilic Normoblast Erythrocyte Erythropoiesis-CPU-E • the committed red cell precursor undergoes several divisions. • The daughter cells becomes progressively smaller, • the cytoplasm changes color from blue to pink as hemoglobin is synthesized, • the nucleus becomes small and dense and then extruded.
Early Intermediate Late Proerythroblast (Pronormoblast) Polychromatophilic Normoblast Reticulocyte Basophilic Normoblast Orthochromatophilic Normoblast Erythrocyte Erythropoiesis-CPU-E • The resulting non-nucleated cells is termed a reticulocyte since it still contains RNA. • Within a few days of entering the circulation, the reticulocytes lose their RNA and becomes mature red cells
Regulation of Erythropoiesis • A. Erythropoietin, • a glycoprotein released predominantly from the kidneys in response to tissue hypoxia. • also produced by reticuloendothelial system of the liver and spleen. • Effect: • a, Stimulates the proliferation and differentiation of the committed red cell precursor • b, Accelerates hemoglobin synthesis • c, Shortens the period of red cell development in the bone marrow.
CONTROL OF ERYTHROPOIESIS: Hypoxia Hypoxia stimulates production of EPOby the kidneys - the tubular epithelial cells and juxtaglomerular cells (90% of EPO) & the liver Biological effects of EPO: 1. ↑ production of proerythroblasts from hematopoietic stem cells 2. ↑ speed of erythropoietic stages ↑ ↑ ↓ Tissue oxygenation is the most powerful regulator of the RBC production (but not the RBC count in the blood)
ERYTHROPOIESIS Morpho-functional changes(proerythroblast → RBC) Appearance of Hb Some Hb is present in the early erythroblasts Late erythroblasts are saturated with Hb Degeneration of the cell organelles Progressive ↓ in the cell size Degeneration of the nucleus Starts in the late erythroblast stage Disappeared by the reticulocyte stage Reticulocytes enter the blood and within 1-2 days develop into mature RBC. Only mature RBC and reticulocytes are present in the blood
RETICULOCYTES & ERYTHROPOIESIS RATE • Normal reticulocytes count in the blood • 1-4% of the circulating RBC in adults • 2-6% in newborns • ↑ reticulocytes count – indicator of rapid RBC production (i.e., hypoxia, hemorrhage, stress, effective therapy of anemia) • ↓ reticulocytes count - ↓ erythropoiesis (↓ EPO production, ↓ ability of red bone marrow to respond to EPO, nutritional anemia, etc.)
CLINICAL FOCUS: BLOOD DOPING AND EPO • Beneficial effects of EPO • ↑ RBC count and O2 carrying capacity of the blood → ↑ O2 delivery to tissues, ↑ muscular performance, ↓ muscular fatigue • Recombinant EPO (rhEPO) is used for treatment of anemias associated with chronic renal failure, AIDS and cancer chemotherapy • Dangers of excessive EPO • Genetically engineered EPO (i.e., darbepoetin) has increased life time • ↑ Htc→ ↑ blood viscosity, ↑ peripheral resistance, ↑ blood pressure, ↓ heart rate (secondary to increased blood pressure), ↑ blood clotting • Genetically engineered EPO often cause production of antibodies against natural EPO and destruction of the RBC
Are required for maturation of the RBC ↑ Synthesis of DNA (synthesis of thymidinetriphosphate– DNA building block) → rapid proliferation of the erythroblastic cells Vitamin B12 (cyanocobolamin) Is required for action of folic acid on erythropoiesis CONTROL OF ERYTHROPOIESIS:Vitamin B12 and folic acid Dietary B12 Parietal/oxyntic cells of gastric mucosa produce intrinsic factor (IF) B12+IF B12 binds with the IF – protection from digestion by GIT secretions Complex of Vit B12 +IF complex binds to the mucosal receptors in the ileum → transport across mucosa Release of B12 into the portal blood freed of IF Binding to the plasma globulins (transcobolamin I, II and III) → red bone marrow or storage in the liver (very large quantities – 3-4 years reserve)
CONTROL OF ERYTHROPOIESIS: Other factors • Testosterone • Stimulates the release of EPO • Adrenal cortical steroids and ACTH • In physiological concentrations stimulate EPOproduction • Large doses are inhibitory
DESTRUCTION OF THE RBC • Sites of destruction • Circulating blood (10% of senescent RBCs) • Macrophage system (spleen and liver) • Senescent RBC • ↓ metabolic rate → ↑ fragility → rupture of the membrane when RBC pass through tight spots of the circulation (i.e., red pulp of the spleen)
METABOLISM OF Hb • Prehepatic • Takes places in themacrophages • Results in formation of bilirubin – a bile pigment • Hepatic • Takes place in the liver (hepatocytes) • Conjugation of bilirubin with glucuronic acid – bilirubin mono- or bi-glucuronideand secretion of conjugated bilirubin into the bile • Posthepatic • Takes place in the GI and kidneys • Formation of urobilinogen and stercobilinogen and excretion
RBC or remnant Macrophages Cell remnants Hemoglobin Hem Globin Pigment Fe++ CO Biliverdin Bilirubin Exhaled • Blood Albumin Bilirubin-albumin Liver Fe++ pool Protein pool PREHEPATIC METABOLISM OF Hb Conversion of the hem pigment into the bile pigment biliverdin+ CO → bilirubin → blood plasma Removal of the globin from Hb in macrophages → protein pool of the body In the plasma water insoluble bilirubin combines with albumin to form water soluble complex → liver
In the liver Replacement of albumin with glucuronic acid – bilirubin mono- or bi-glucuronide (water soluble) Excretion of conjugated bilirubin into the small intestine via the bile In the small intestine Conversion of bilirubin to urobilinogen by the intestinal bacteria Conversion to stercobilinogen→ oxidationand excretion in the feces as stercobilin Absorption from the small intestine & either re-excretion by the liver or oxidation & excretion by the kidneys as urobilin. Liver Glucuronic acid Albumin Bilirubin-glucuronide Urobilinogen(in the small intestine) Reabsorption Stercobilinogen Re-excretion in bile Excretion as urobilin in urine Excretion as stercobilin in feces HEPATIC & POSTHEPATIC METABOLISM OF BILIRUBIN Transport of bilirubin from plasma into the hepatocytes
JAUNDICE Refers to the yellow color of the skin, conjunctivae and mucous membranes caused by the presence of excessive bilirubin in the plasma and body fluids (jaune(French) = yellow) Blood bilirubin level must exceed three times the normal values, for the coloration to be easy visible • Types of jaundice: • Pre-hepatic – the pathology occurs prior to the liver • Hepatic– the pathology is located in the liver • Post-hepatic – the pathology occurs after the conjugation of bilirubin in the liver
PRE-HEPATIC JAUNDICE Excessive hemolysis of the RBCs – hemolytic jaundice • bilirubin production ↑ unconjugated(indirect)bilirubin Capacity of the liver to conjugate bilirubin is exceeded (saturation of enzyme glucuronyl transferase) Normal conjugated (direct) bilirubin N urobilinogen formation urobilinogen → dark urine ↑ stercobilinogen → dark feces
HEPATIC JAUNDICE Results from infective or toxic damage to the liver cells (hepatocellular damage) Uptake, conjugation and/or excretion of bilirubin is affected ↑ unconjugated bilirubin Normal/decreased conjugated bilirubin ↑ urobilinogen in blood (↓ enterohepatic circulation and hepatic extraction of blood urobilinogen by damaged hepatocytes) ↑ urobilinogen filtration and excretion in urine Pale/N stool Dark urine
POSTHEPATIC JAUNDICE Results from obstruction of the bile ducts by stones, tumors, etc. Functioning of the hepatic cells is normal N Normal unconjugated bilirubin plasma level of conjugated bilirubin due to the bile entry into the blood from ruptured congested canaliculi and ↑ total bilirubin urobilinogen formation Conjugated bilirubin in urine (kidney can excrete small quantities of highly soluble conjugated bilirubin) → dark urine ↓ or absent urobilin in urine ↓ stercobilin content in feces → pale feces
Hemolysis of the excess RBC when the infant is suddenly exposed to a high oxygen environment and hence does not need so many RBC as in the uterus Immaturity of the liver (inability to conjugate significant quantities of bilirubin with glucuronic acid for excretion into the bile) to handle the excess bilirubin (especially in premature babies) ↑ plasma total bilirubin concentration (less than 1 mg/dL → 5 mg/dL) Mild jaundice (yellowness) of the infant’s skin and the sclerae for 1-2 weeks PHYSIOLOGICAL JAUNDICE OF THE NEWBORN
IRON METABOLISM • Dissociation of Fe from the hem→ plasma → binding to transferrin, transport in the blood → • Detachment from transferrin & storage in the liver, muscle cells & macrophages attached to ferritin or hemosiderin→ • Release from the storage sites, transport in the blood by transferrin • Transport into the RBC precursor cells by receptor mediated endocytosis → Hem synthesis 2 1 3 4 ↓ quantities of transferrin → ↓ Hb content in the RBC – hypochromic anemia Synthesis of transferrin increases with iron deficiency but decreases with any type of chronic disease.
FORMS OF IRON IN THE BODY • Recommended daily intake - 15 – 18 mg (250-330 μmol) • Minimal absorption to balance iron loss • Adult males - 35 μmol • Adult females - 175 μmol • Distribution of body iron in an average man • Hb, 2100 mg • Ferritin - water soluble protein-iron complex , 700 mg (in theliver, spleen, marrow and plasma) • Hemosiderin - water insoluble complex (macrophages of the liver and bone marrow), 300 mg • Myoglobin - local oxygen reserve, 200 mg • Tissue (heme and nonheme) enzymes, 150 mg • Transport-iron compartment in plasma (transferrin), 3 mg.
HEMOCHROMATOSIS • Reasons • Primary - one of the most common autosomal recessive genetic disorders characterized by excessive absorption of dietary iron resulting in a pathological increase in total body iron stores • Failure to reduce iron reabsorption in response to increased iron level in the body • Secondary – is not genetic (results from anemia, alcoholism, transfusion iron overload –hemosiderosis, etc.) • Consequences • Deposition of iron in the body tissues (liver, heart, pancreas, pituitary, joints, and skin) initially as ferritin and than as hemosiderin • Toxic action on organs and damage of cells due to action as a pro-oxidant (↑ formation of free radical formation, i.e., the hydroxyl radical and the superoxide radical) → DNA cleavage, impaired protein synthesis, and impairment of cell integrity and cell proliferation, leading to cell injury and fibrosis. • Cirrhosis, hyperpigmentation of skin, diabetes mellitus, impotence, joint diseases, etc.
Specific weight of the RBC is higher than that of the plasma in a stabilized blood, RBC slowly sink towards the bottom of the test tube -sedimentation Factors increasing ESR ↓ Htc, ↓ blood viscosity ↑ concentration of fibrinogen (i.e., pregnancy, vascular diseases, heart diseases), haptoglobulin, lipoproteins, immunoglobulins Macrocytic RBC Extreme elevation of WBC count (leukemia) Factors decreasing ESR ↑ Htc Change in the RBC shape (i.e., sickle-cell anemia, poikilocytosis – nonuniformity of shape) ↑ albumin concentration ESR Clumps of RBCs ERYTHROCYTE SEDIMENTATION RATE (ESR) Males – 3-6 mm/h Females – 8-10 mm/h
ANEMIA • Deficiency of blood Hb due to • ↓ RBC count (too rapid loss or/and too slow production) • ↓ Hb quantity in the RBC WHO's Hemoglobin thresholds used to define anemia (1 g/dL = 0.6206 mmol/L)
ANEMIA: CONSEQUENCES • ↓ oxygen-carrying capacity of the blood → hypoxia → vasodilation • ↑ in pulse and respiratory rates (effort to supply sufficient oxygen to tissues) • ↓ exercise & cold tolerance • Pale skin (↓ red colored oxyHb) • ↑ fatigue and lassitude • ↓ blood viscosity → ↓ peripheral vascular resistance → ↑ blood flow, venous return, cardiac output and work load on the heart
ANEMIAS: Classifications Anemia: classification according to MCV Classification according to etiological ground • Nutritional • Aplastic • Hemorrhagic • Hemolytic Macrocytic anemia (MCV>100) Normocytic anemia (80<MCV<100) Microcytic anemia(MCV<80) Deficiency of vit B12, folic acid,or IF. Hypothyroidism.Alcoholism. Liver diseases. Drugs that inhibit DNA replication (i.e., methotrexate, zidovudine) Hem synthesis defect (i.e., iron deficiency, chronic diseases) Globin synthesis defect (i.e., thalassemia) Sideroblastic defect Acute blood loss, chronic diseases, bone marrow failure, hemolysis
Iron deficiency Is the most common type Reasons Premenopousal women: Blood loss during menses(20% of all women of childbearing age have iron deficiency anemia, compared with only 2% of adult men) Males and postmenopausal females: Excessive iron loss due to chronic occult bleeding (peptic ulcer, tumor, etc.) Increased iron demands (i.e., pregnancy and lactation) Inadequate iron intake or absorption (i.e., vit. C deficiency) Parasitic infestation(hookworm, amebiasis, schistosomiasis) Chronic intravascular hemolysis (if the amount of iron released during hemolysis exceeds the plasma iron-binding capacity) ANEMIA: Nutritional
IRON DEFICIENCY ANEMIA: CONSEQUENCES • Low serum ferritin (serum iron) level • Plasma ferritin concentration is an excellent indicator of the iron stored in the body, because of a dynamic balance between intra- and extracellular ferritin iron • ↓ bone marrow iron stores (ferritin and hemosiderin) • ↓ saturation of transferrin • ↓ RBC count & Htc • RBC are small and look pale - microcytic hypochromic anemia • Abnormal fissuring of the angular (corner) sections of the lips (angular stomatitis). • Abnormal craving to eat substances(eg, ice, dirt, paint).
DEFICIENCY OF IRON UTILIZATION: SIDEROBLASTIC ANEMIA • Inadequate marrow utilization of iron for Hb synthesis despite the presence of adequate or increased amounts of iron • Reasons:Hereditary oracquired, including lead and ethanol toxicity, pyridoxine deficiency • Deficient reticulocyte production, intramedullary death of RBCs, and bone marrow erythroid hyperplasia (and dysplasia) • Presence of polychromatophilic, stippled RBCs (siderocytes) • Hipochromic, microcytic RBCs, variations in RBC size Ring sideroblasts are erythroid precursors whose mitochondria (located around the nucleus) are loaded with nonheme iron.
ANEMIA: Nutritional (cont.) Deficiency of vitamin B12 and/or folic acid • Reasons • Inadequate intake (a strict vegetarian diet excluding all meat, fish, dairy products, and eggs; chronic alcoholism) • Inadequate GI absorption • Lack of IF - pernicious anemia • Autoimmune destruction of parietal cells (atrophic gastric mucosa) or AB against IF • Removal of the functional portion of the stomach, such as during gastric bypass surgery • Crohn's disease intestinal malabsorption disorders • Resection (or inflammation) of the ileum(site of B12 reabsorption) • Consequences • Maturation failure • Failure of DNA synthesis with preserved RNA synthesis, which result in restricted cell division of the progenitor cells. • Production of large precursor cells – megaloblasts and larger irregular oval erythrocytes – macrocytes fully saturated with Hb –macrocytic (megaloblastic) anemia • ↑ fragility of the plasma membrane → ↓ life span → anemia • Vitamin B12 deficiency only results in peripheral neuropathy and spinal cord degeneration