Download
1 / 15
150 likes | 159 Views
Explore the complexities of mental disorders and the challenges in defining and diagnosing them. Learn about the criteria, stigma, gender bias, and societal impact on individuals with different disorders.

E N D
Do Now Does Moondog have a psychological disorder? This is Moondog. As a blind poet and musician, he stood on street corners in Manhattan for over three decades, dressed like this. He made enough money to live on by selling copies of his poems and homemade instruments to passersby. Although his behavior was unusual, there was no evidence that it caused himself harm or distress. In fact, he used to say that the people who force themselves to adapt to the expectations of modern society are the ones who are truly distressed. Do you think that Moondog has a mental illness? Why or why not?
Personality and Disorders • Connections • All of us are sad or depressed for short periods every once in a while. • All of us are anxious sometimes • These are adaptive emotions, in that they motivate us to change things or avoid danger • Lots of variability in the normal range • However, for several people, anxiety or depression in moderation gives way to severe levels of these emotions, which can be maladaptive
Criteria for mental disorders Mental disorders are suggested when associated behaviors… • are inappropriate to current context • are "extreme“ in prevalence or nature • cause person distress • are uncontrollable • violate expectations of the observers or society
How do psychologists define mental disorder? Diagnosis and categorization key According to DSM-IV, a mental disorder is a set of actions, thoughts, and feelings (symptoms) that: 1) poses Clinically Significant Detriment - Detriment = distress, or impairment of functioning in daily life - Clinically Significant = the detriment must be serious enough to be treated 2) has an Internal Source - The distress or impairment must be in a person’s biology, mental structure, or habits. - A mental disorder can not be an expected reaction to life’s circumstances or environment. 3) shows Involuntary Manifestation - The symptoms of a mental disorder must not be voluntary.
Why are mental disorders so difficult to define? • Many symptoms of mental illness are difficult to measure and can be interpreted in many ways. • It is difficult to create a classification system for mental illness that is reliable and valid. • Reliability -- the degree to which psychologists agree that a disorder is present • Validity -- the degree to which a person’s symptoms are correctly classified • The DSM-IV is the most accurate manual to date because it uses observable characteristics and self-descriptions and does not rely on data that could cause disagreement among psychologists. • Disorders can be influenced by cultural factors (anorexia).
Gender bias in diagnosis • Dependence on self-report • Men usually report less anxiety. • Acceptability of emotions • There is a higher social acceptability of men developing dependencies that mask problem, which might masks other mood disorders • Psychologist diagnosis and gender (Ford & Widiger, 1989) • similar cases sent to psychologists • IV: male or female, type of cause • DV: diagnosis • R: women labeled “histrionic personality” while men labeled “antisocial personality” • Based on supposed frequencies with a population
Stigma of mentally ill label • Changes other’s behavior • Harris et al. (1992) - grade school boys more rejecting of other boys if told they had been diagnosed with ADHD • Langer & Abelson (1974) - man discussing his personal problems – subjects rated him more negatively if told he was a mental patient • Changes own behavior • Farina, et al. (1971) – ex-mental patients acted more anxious when believed that interviewer knew of their patient status • The importance of labeling has lead to debate about what language is used to describe mental disorders, particularly when it comes to describing a person’s agency or control of the disorder • person suffering from schizophrenia” instead of “a schizophrenic” • Stable (internal) or unstable (environmental)
Medical Student Disease(AP Psychology Disease) • Strong tendency to find in oneself or one’s surroundings the symptoms or concepts discussed in school at an absurd rate • “I had walked into that reading-room a happy, healthy man. I crawled out a decrepit wreck” - Jerome K. Jerome • The reason is everyone has one symptom or another • Notice DSM-IV states all need to be present for valid diagnosis
Expectancy Effects with Mental Disorders - Rosenhan (1973) sent 8 pseudo patients to a local asylum. All reported one symptom, auditory hallucination (I hear voices that say, “Empty, hollow, thud.”). They were instructed to behave normally after admission - No staff member detected the pseudo patients but other patients did - Staff reinterpreted behavior to fit context and diagnosis - “intellectualization defense” - “writing behavior” - Discharge diagnosis: Schizophrenia in remission
Perspectives How do psychologists of different perspectives DISAGREE about the nature of mental illness?
How do psychologists of different perspectives DISAGREE about the nature of mental illness?
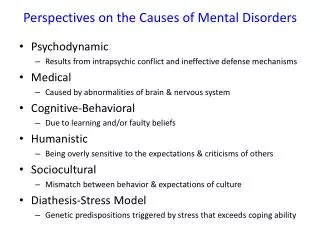
Commonalities Between Perspectives on Disorders Psychologists of all perspectives realize that disorders have multiple causes. • Predisposing Causes - influences that exist before the disorder begins and makes people vulnerable to the disorder. • Ex. genetics, socio-cultural values, patterns of beliefs and habits. • Diathesis/stress • Individuals born with predispositions (diatheses), but not always realized - only when system stressed • Precipitating Causes - events that bring about a disorder (stresses). Losses, threats, or changes can bring about disorders. • Ex. death of loved one, threats to health, divorce, any large change in daily life. When people have related predisposing causes, disorders can result. • Maintaining Causes - consequences of a disorder that make the disorder more likely to continue. • Ex. increased attention, withdrawal/ rejection of friends, strange sleep patterns